









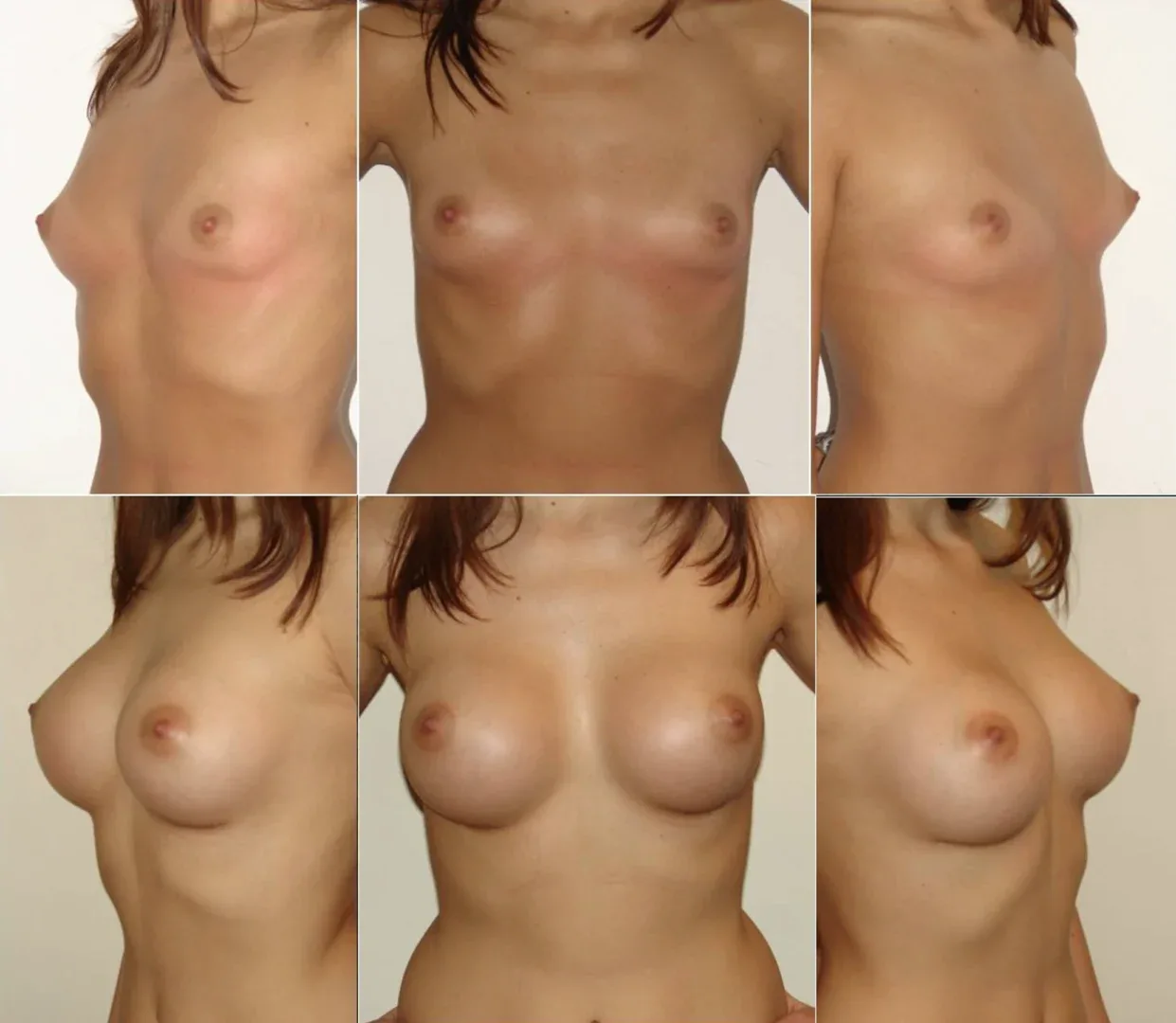
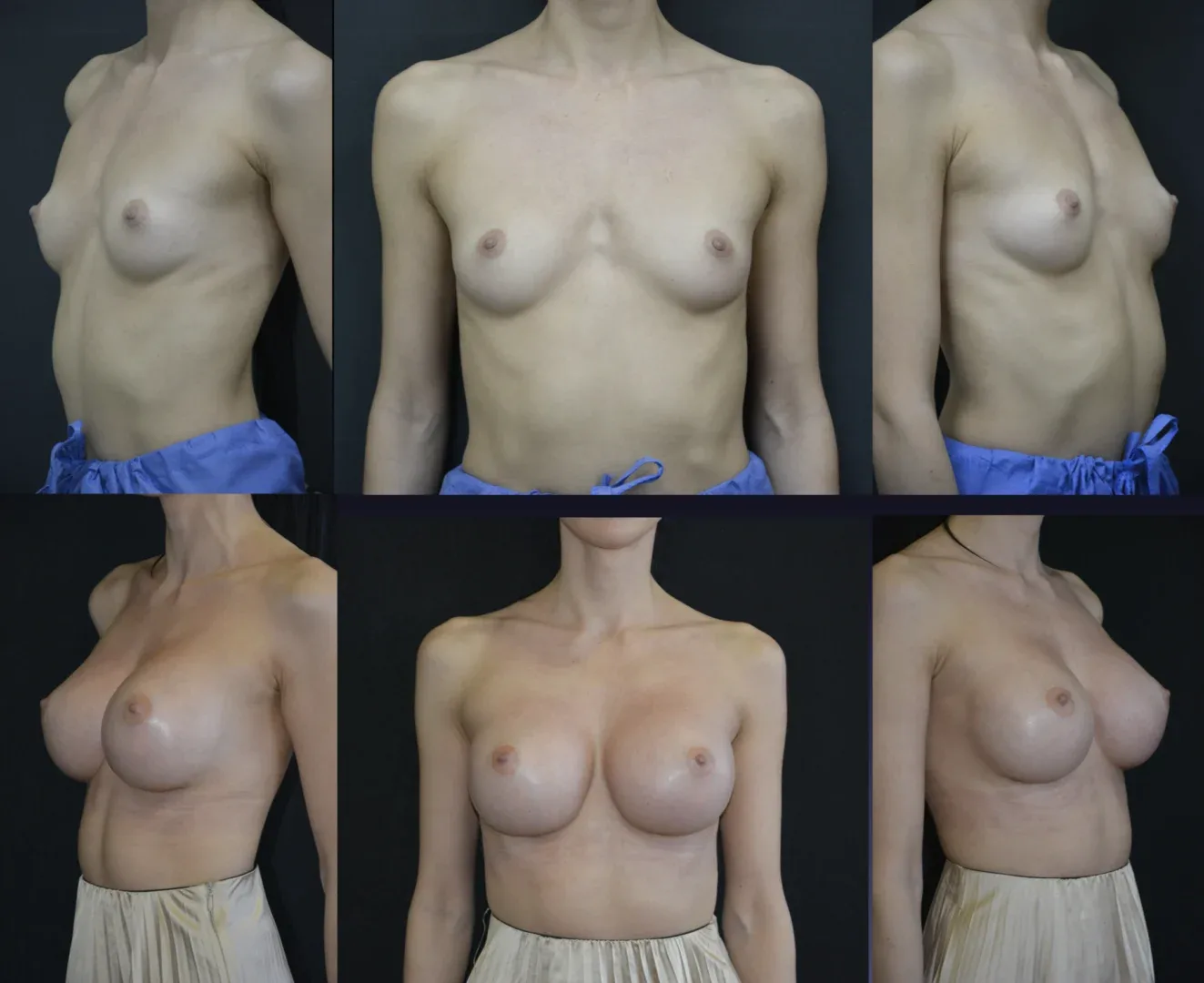
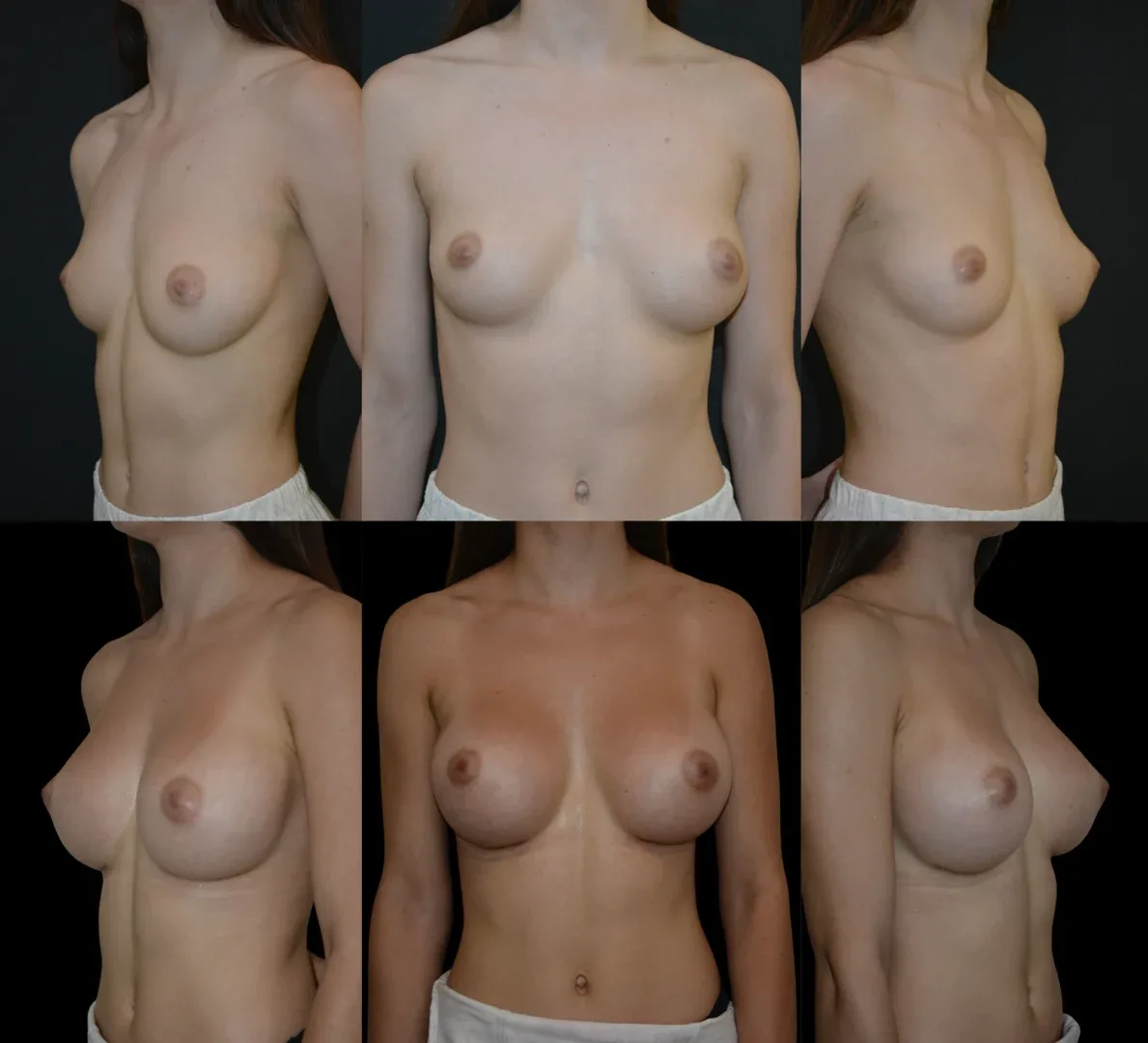
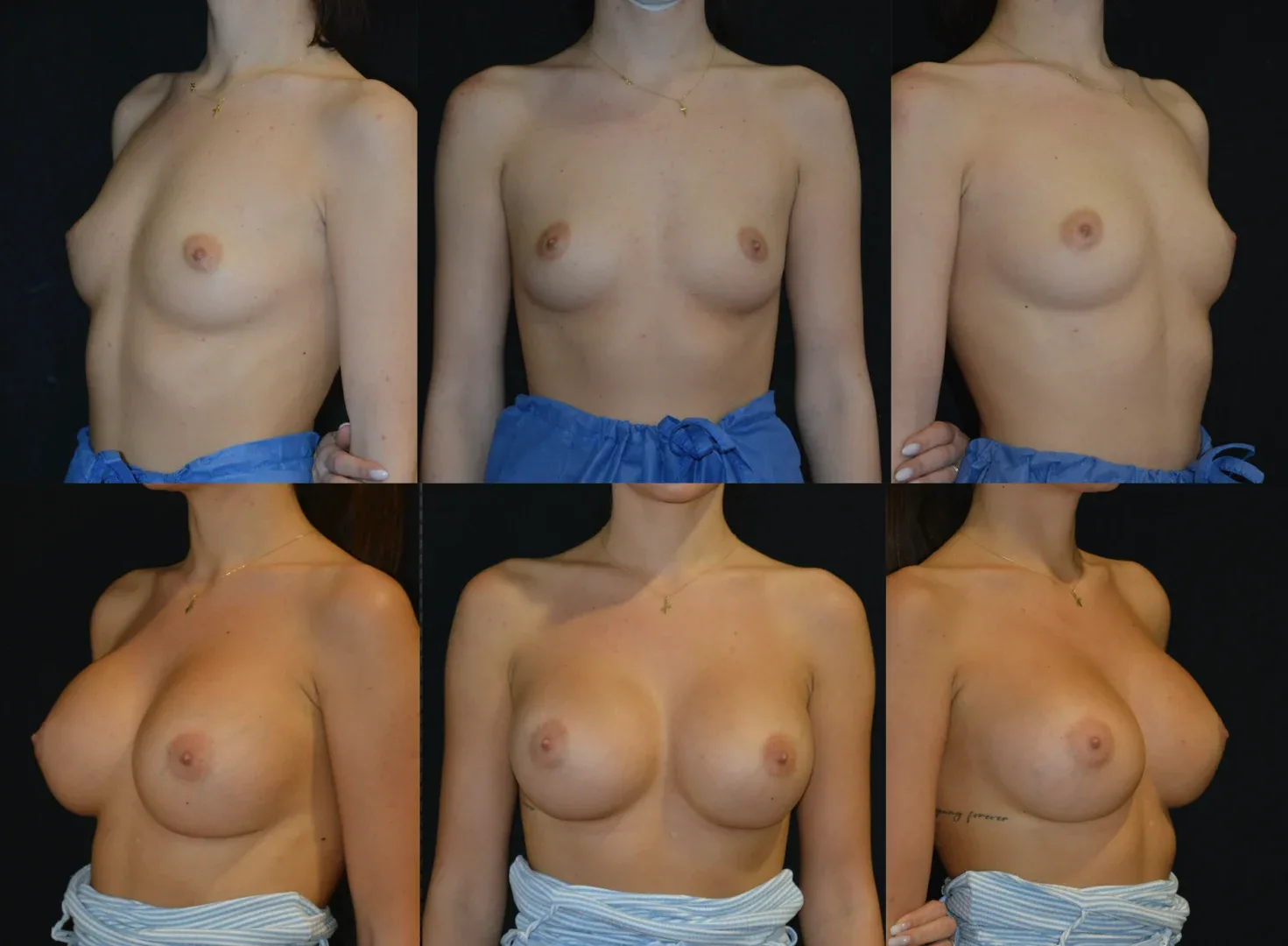
Breast augmentation is performed using breast implants to increase the volume and projection of the breasts or to achieve symmetry; it is used for:
- Breast enlargement
- Restoration of breast volume and firmness after pregnancy or weight loss
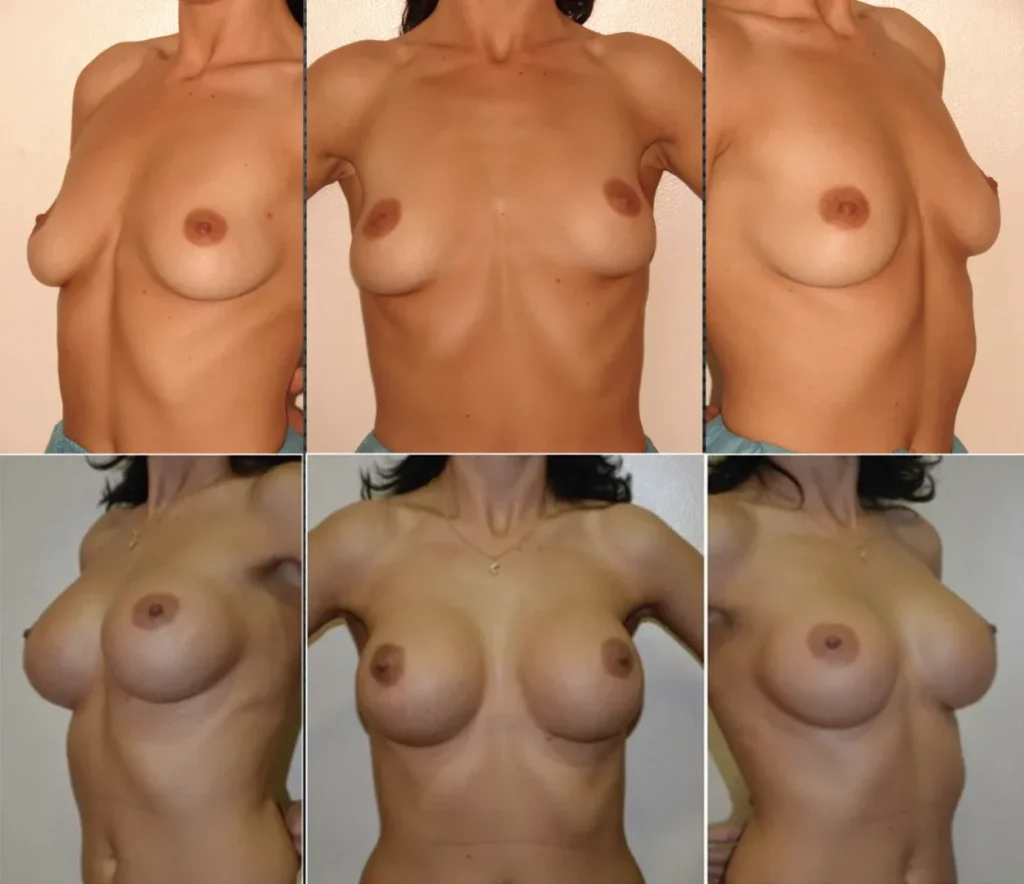
- Achieving breast symmetry in terms of shape and size
- Breast augmentation does not correct sagging breasts; if the goal is both enlargement and correction of the position and shape of sagging breasts, a breast lift (internal and/or classic mastopexy) must be performed simultaneously with augmentation.
Adult women, regardless of age, can benefit from breast augmentation to increase breast volume or restore firmness. It is recommended that the breast be fully developed before undergoing the procedure. Generally, breast augmentation does not affect breastfeeding.
A woman motivated by her own desire to have larger breasts is usually satisfied with the results of breast augmentation. The best candidates for this procedure are:
- Healthy patients without conditions affecting healing
- Non-smokers
- Individuals with a pleasant appearance who specifically wish to improve their body aesthetics
The success, safety, and results of breast augmentation require that:
- The patient communicates her wishes openly with the plastic surgeon
- Medical history, medication use, vitamins, natural supplements, alcohol, tobacco, drugs, diets (weight-loss or vegetarian/vegan) must be openly discussed with the doctor
- The doctor is informed about any family history of breast cancer
- The patient follows the surgeon’s instructions exactly
Breast augmentation is performed using biocompatible breast implants (prostheses), with smooth or textured surfaces, filled with silicone gel. Implant placement, type, and volume are determined based on breast type, body shape, measurements taken during consultation, the patient’s wishes, and the surgeon’s experience.
In subglandular placement (under the mammary gland), the implant edges may be visible and the incidence of capsular contracture is higher.
In submuscular augmentation (under the pectoral muscle), the implant edges are better concealed, but the implant may shift due to muscle contractions, and recovery is longer (postoperative pain is greater).
Subfascial augmentation (implant placed under the pectoral fascia) combines the advantages of both techniques (subglandular and submuscular) without their disadvantages, being more predictable and stable long-term, especially after major body weight changes such as pregnancy. Comparative studies show that submuscular augmentation has 3–5 times higher rates of complications (capsular contracture, malposition, implant displacement, double bubble).
SUBFASCIAL TECHNIQUE (see details)
When subpectoral implant placement is recommended (e.g., when internal lifting techniques are combined), I use the muscle splitting biplane technique. Here, the pectoral muscle is not detached from the chest wall but split along its fibers. This minimizes breast distortion during muscle contraction, reduces the gap between breasts, lowers the risk of double bubble, and decreases postoperative pain compared to the dual-plane or classic submuscular technique.
MUSCLE SPLITTING BIPLANE TECHNIQUE and INTERNAL LIFT TYPE 1 TECHNIQUE (see details)
Breast implants do not affect breast health. There is no evidence linking implants to autoimmune diseases, systemic illnesses, or breast cancer. However, implants may alter the breast’s appearance and feel. Capsular contracture — a fibrotic capsule deforming the breast — can occur and may require surgical correction, though results may not be permanent.
Breast implants are not lifetime devices, and future replacement surgery may be required. Pregnancy, weight changes, and menopause can affect their appearance over time.
Before augmentation, a breast ultrasound or mammogram is recommended to assess breast health and for future comparison. After augmentation, mammography becomes technically difficult and may risk implant rupture. Women with implants should always inform their doctor before breast examinations.
Possible risks include bleeding, infection, poor incision healing, scarring, and nipple or breast sensitivity changes (usually temporary). Capsular contracture may also occur, requiring surgery. As with any operation, anesthesia risks are present.
Surgeries are performed using the PenEvac™ – Crystal Vision™ system (I.C. Medical, USA), an advanced electrocautery with telescopic extension and smoke filtration. This ensures excellent intraoperative visibility, hemostasis, reduced bleeding, and fewer postoperative complications (bleeding, hematomas, infections). Smoke evacuation also minimizes swelling, pain, and recovery time.
After surgery, incisions are dressed and a special bra (support garment) is applied to reduce swelling, support the breasts, and aid healing.
Initial healing includes swelling, inflammation, and discomfort at incision and breast level. Pain is controlled with medication. Wearing the bra for several weeks is recommended. Return to light activities is possible 1–2 days post-surgery.
Initial wound healing takes 1–2 weeks. The patient may resume work and normal activities as long as no physical effort is involved.
Healing continues over the following weeks, during which swelling decreases, implants settle, and scars fade; incision lines, though permanent, become barely visible.
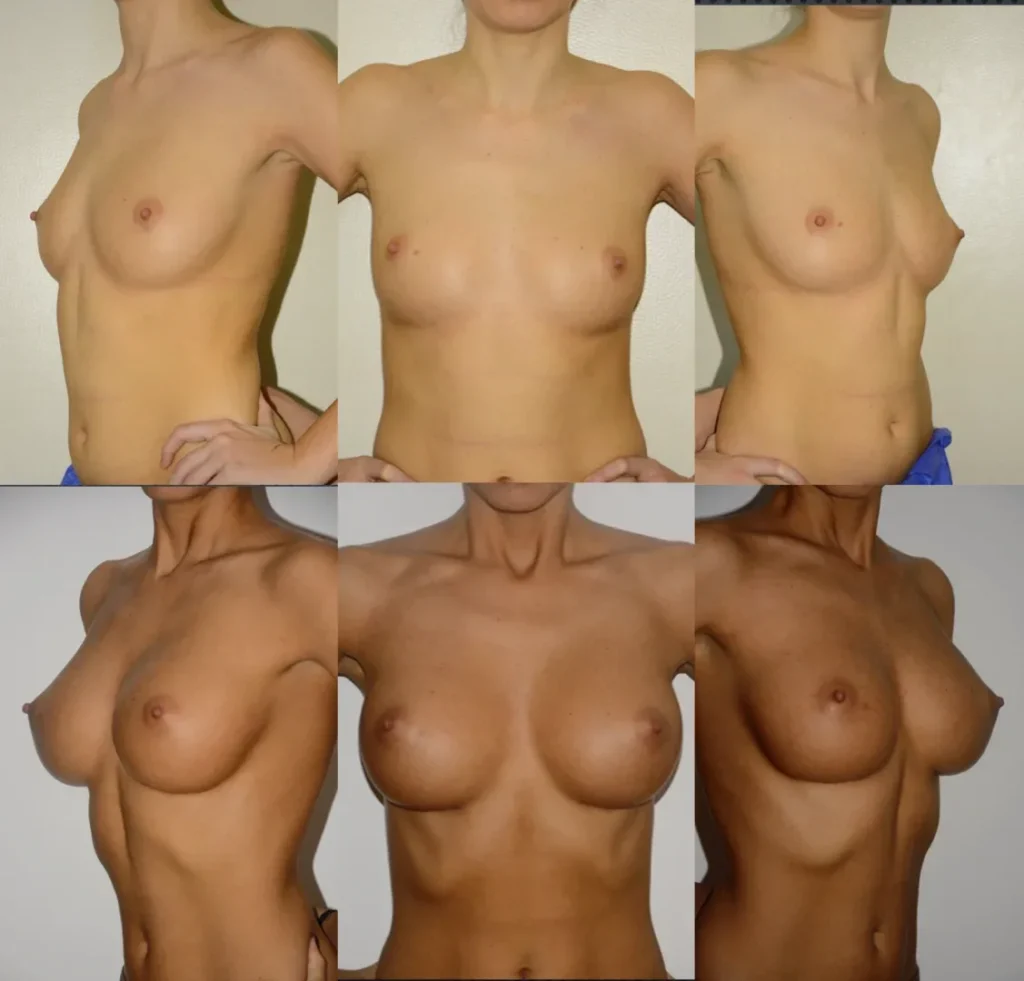
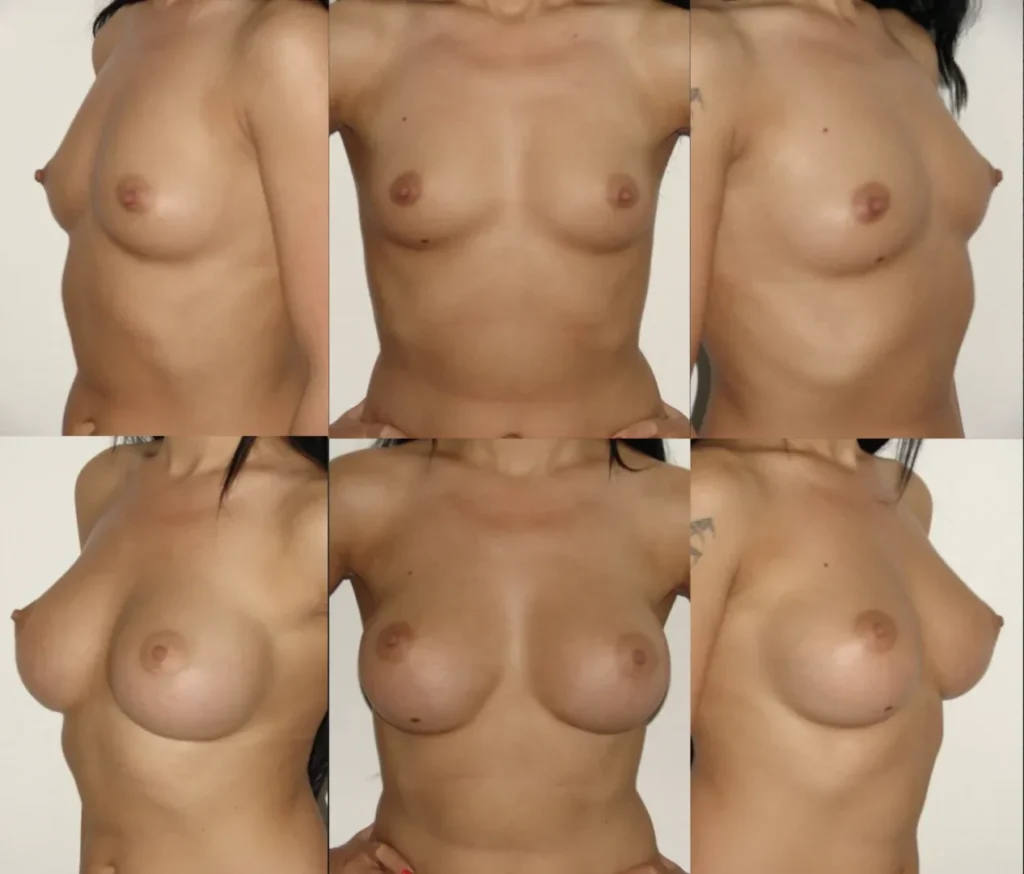
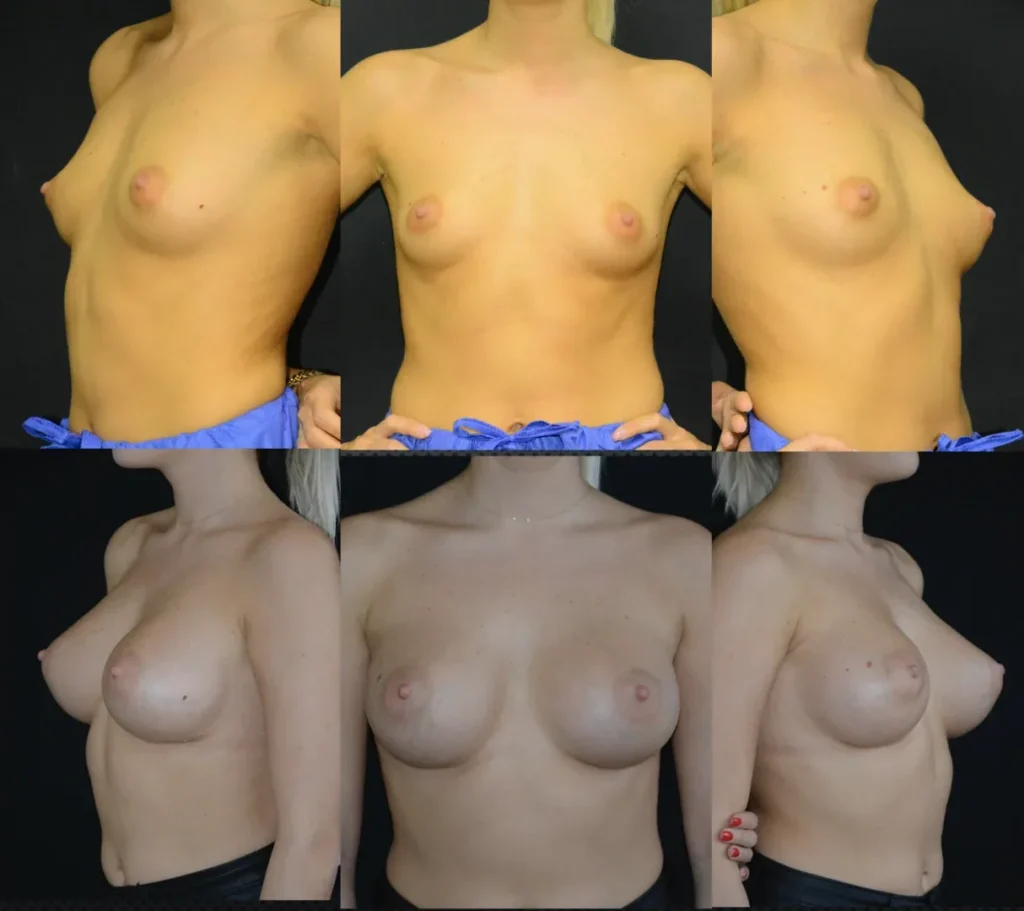
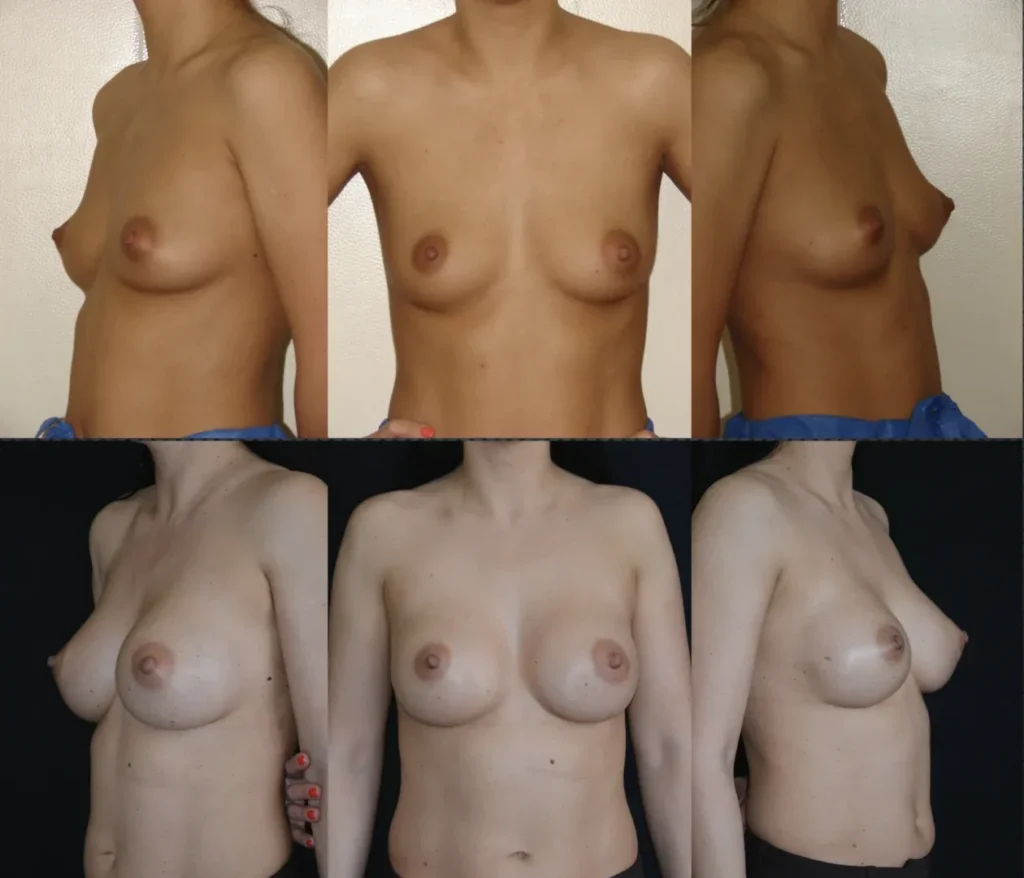
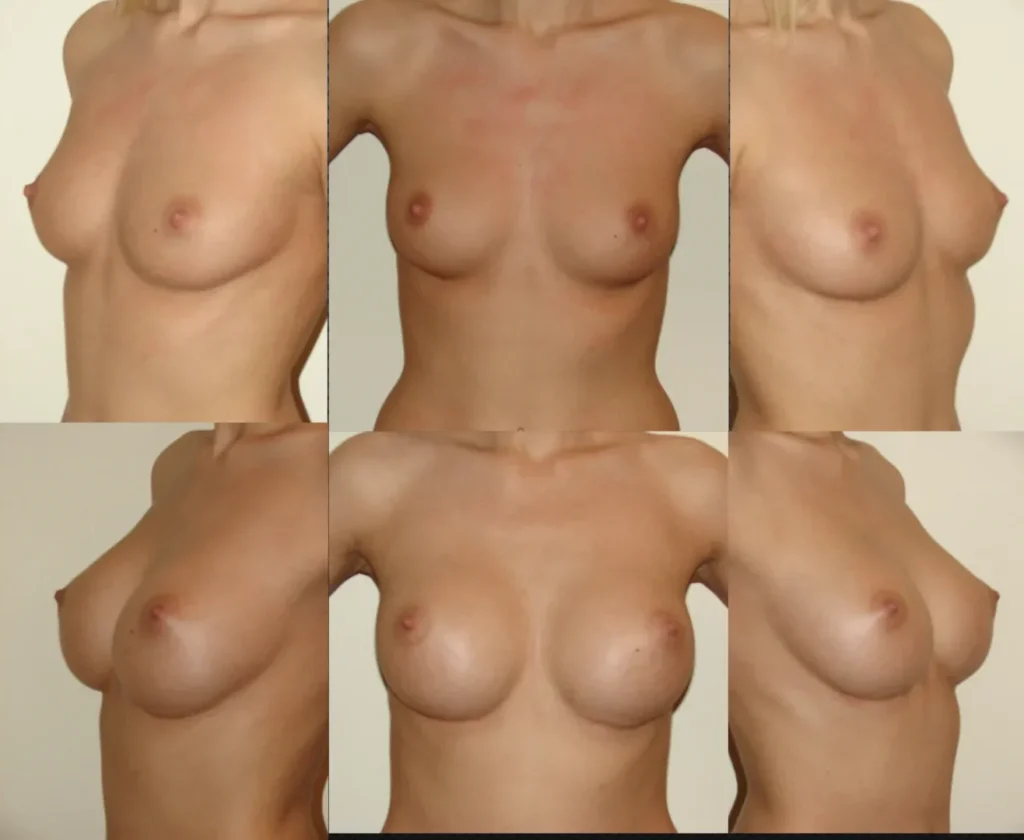
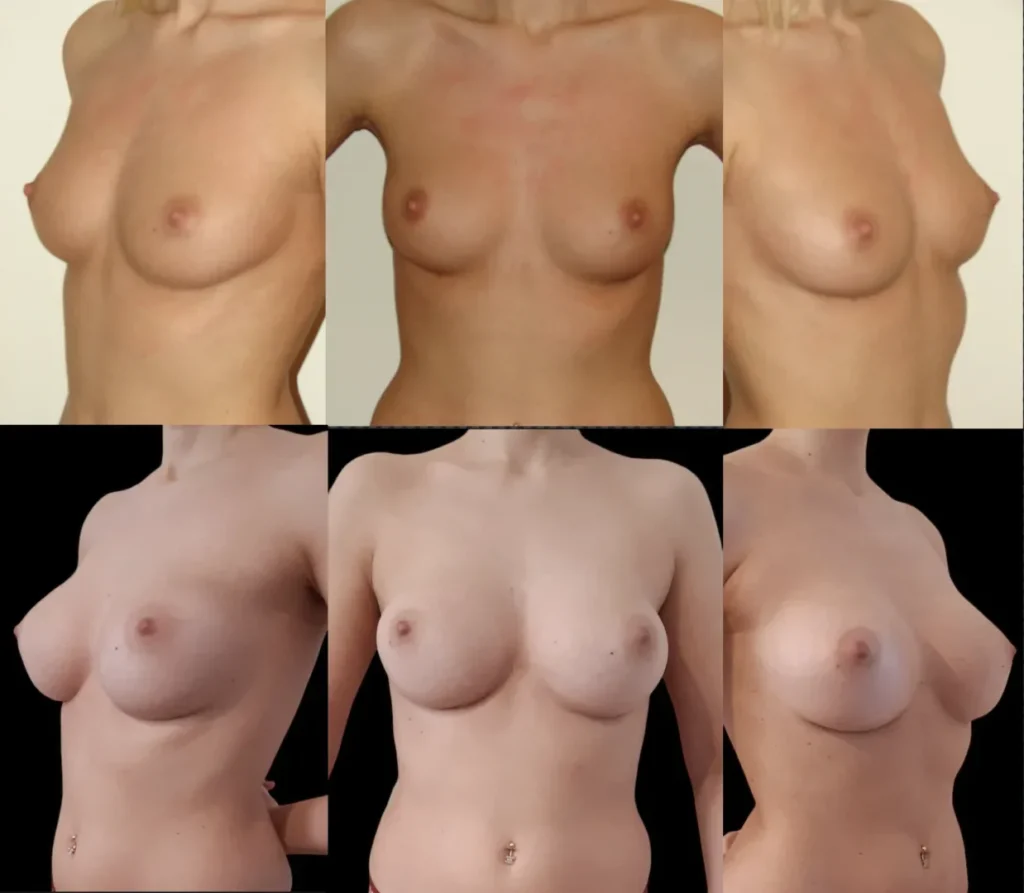
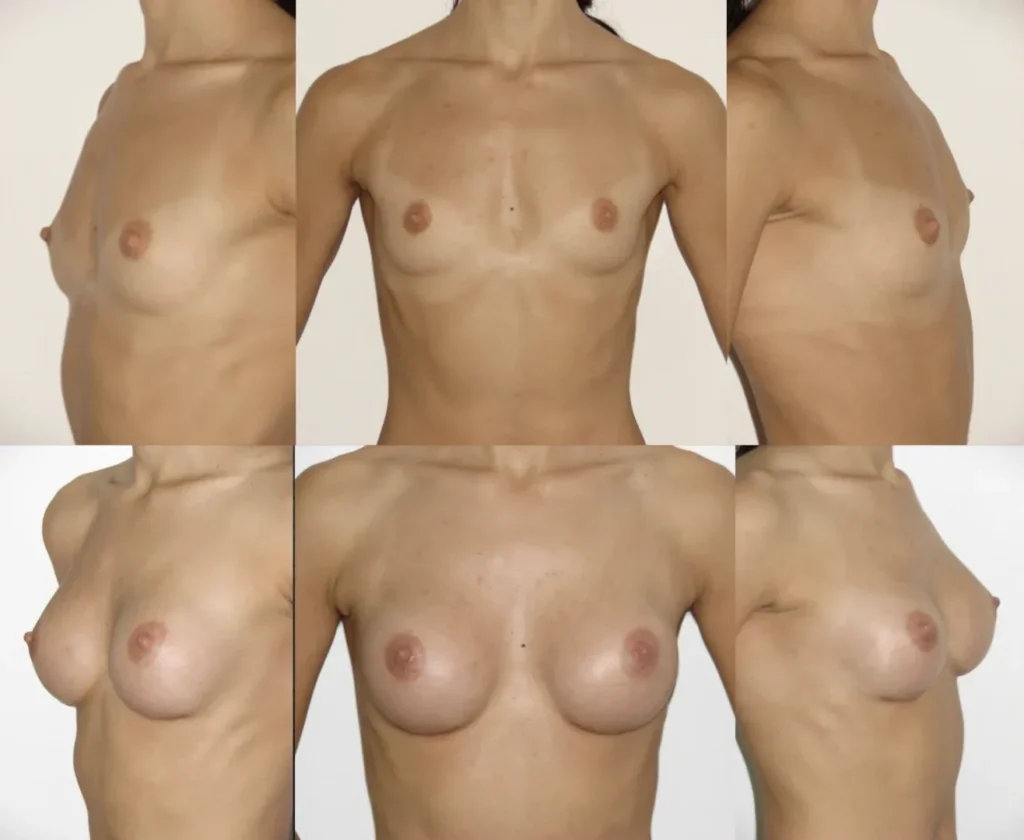
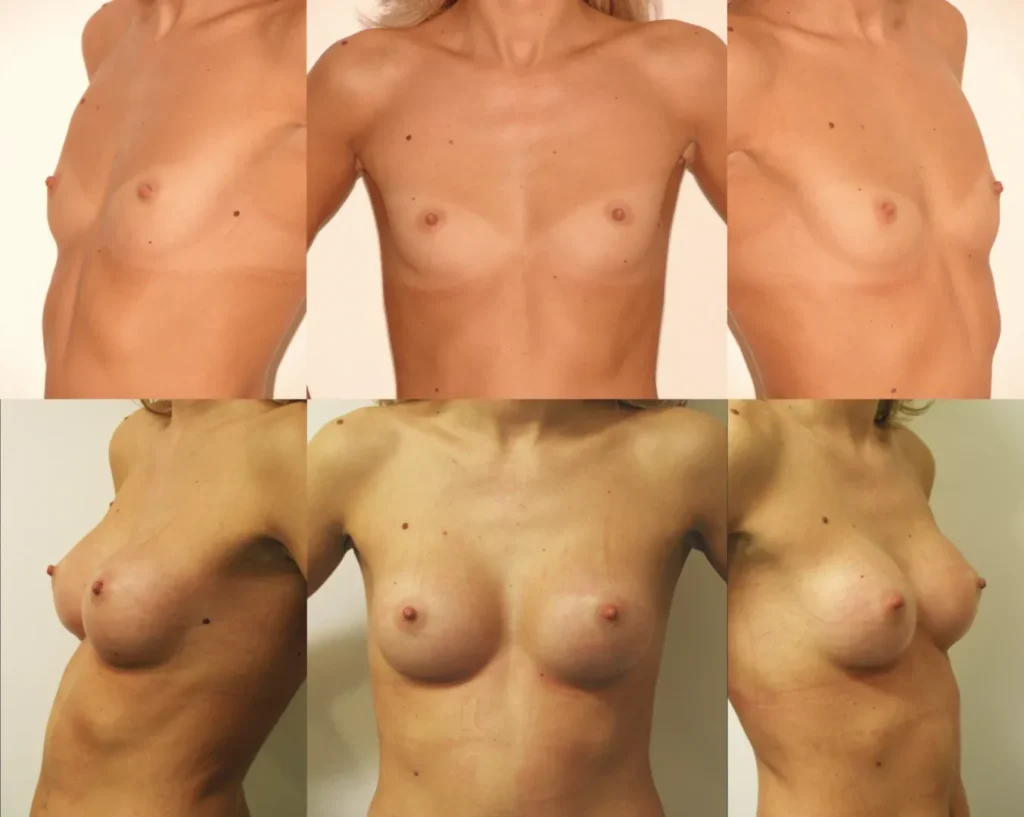
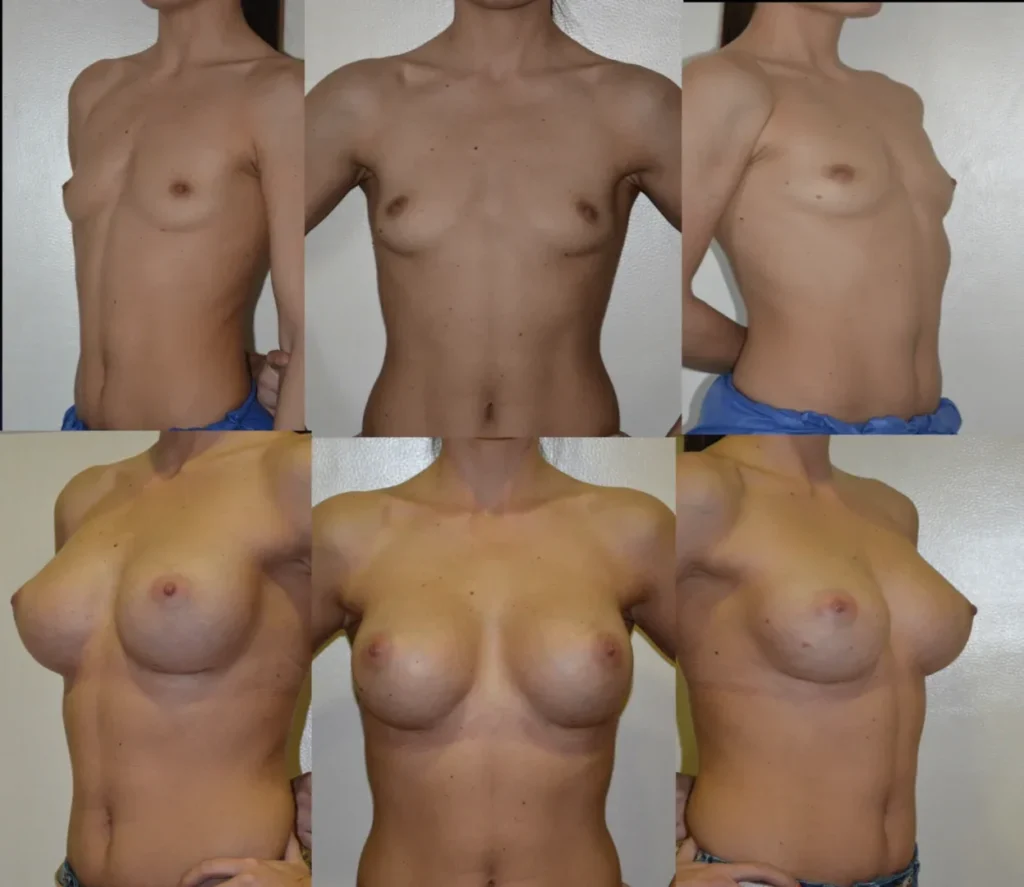
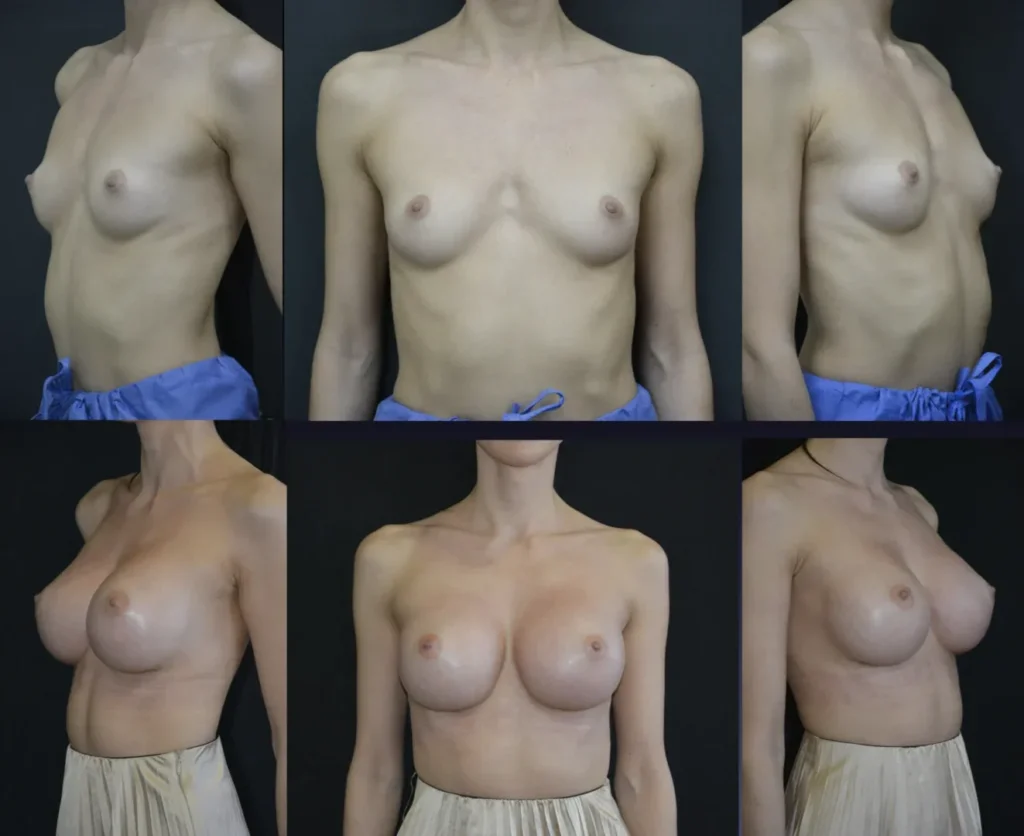
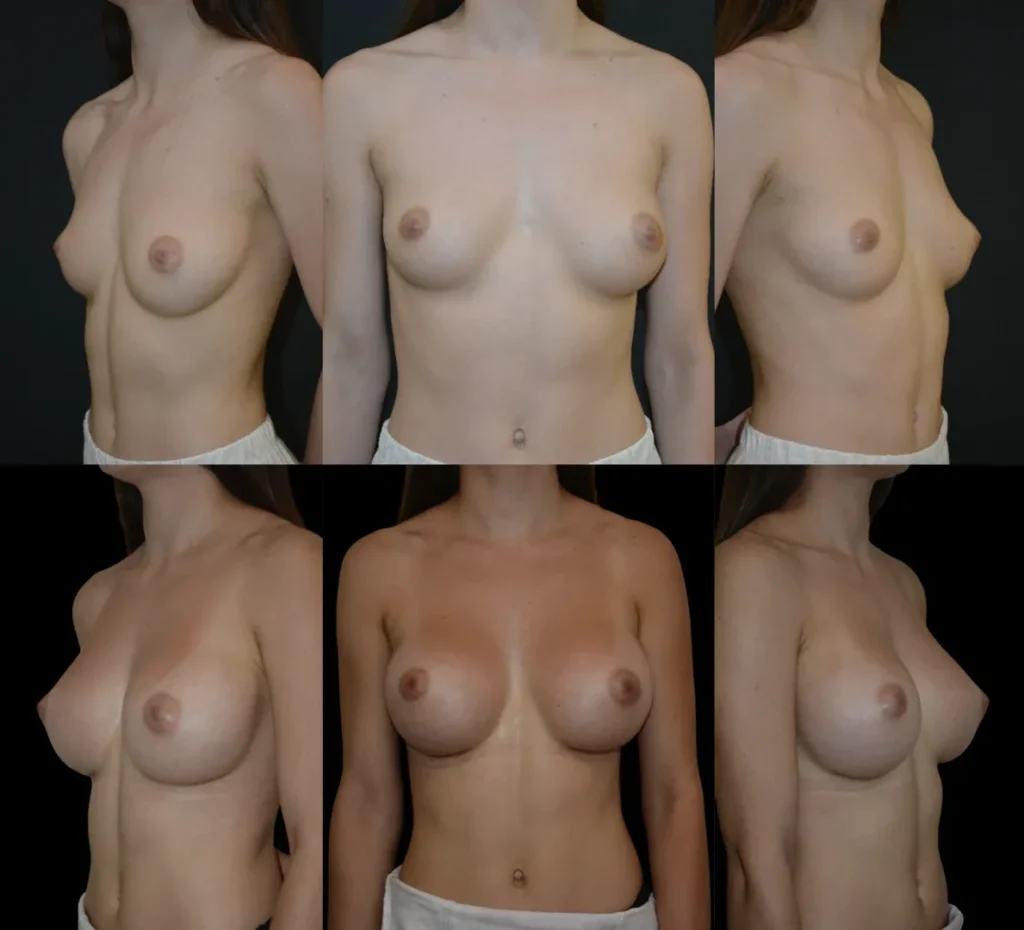
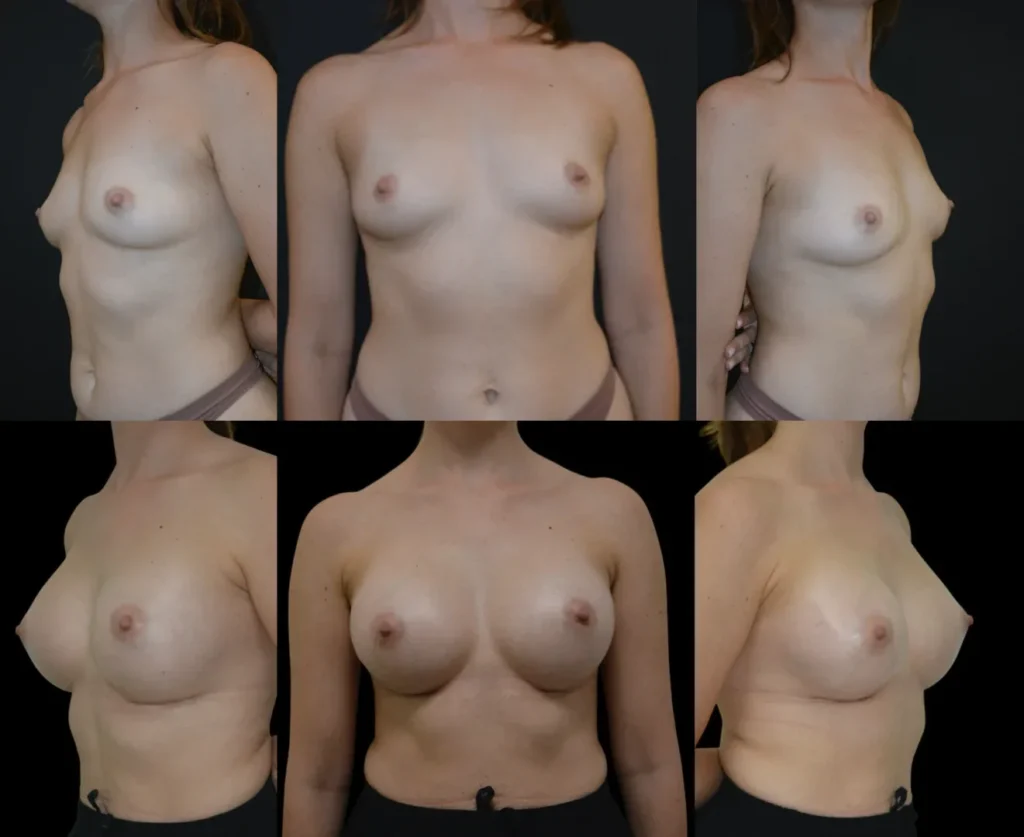
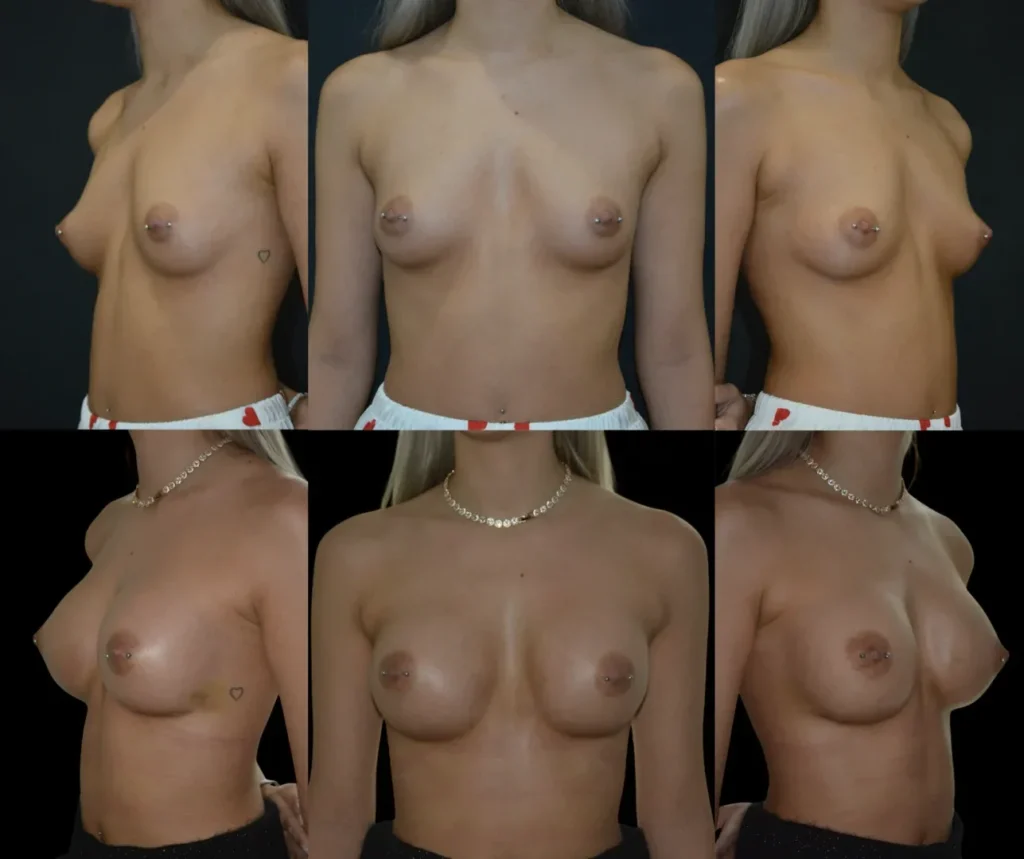
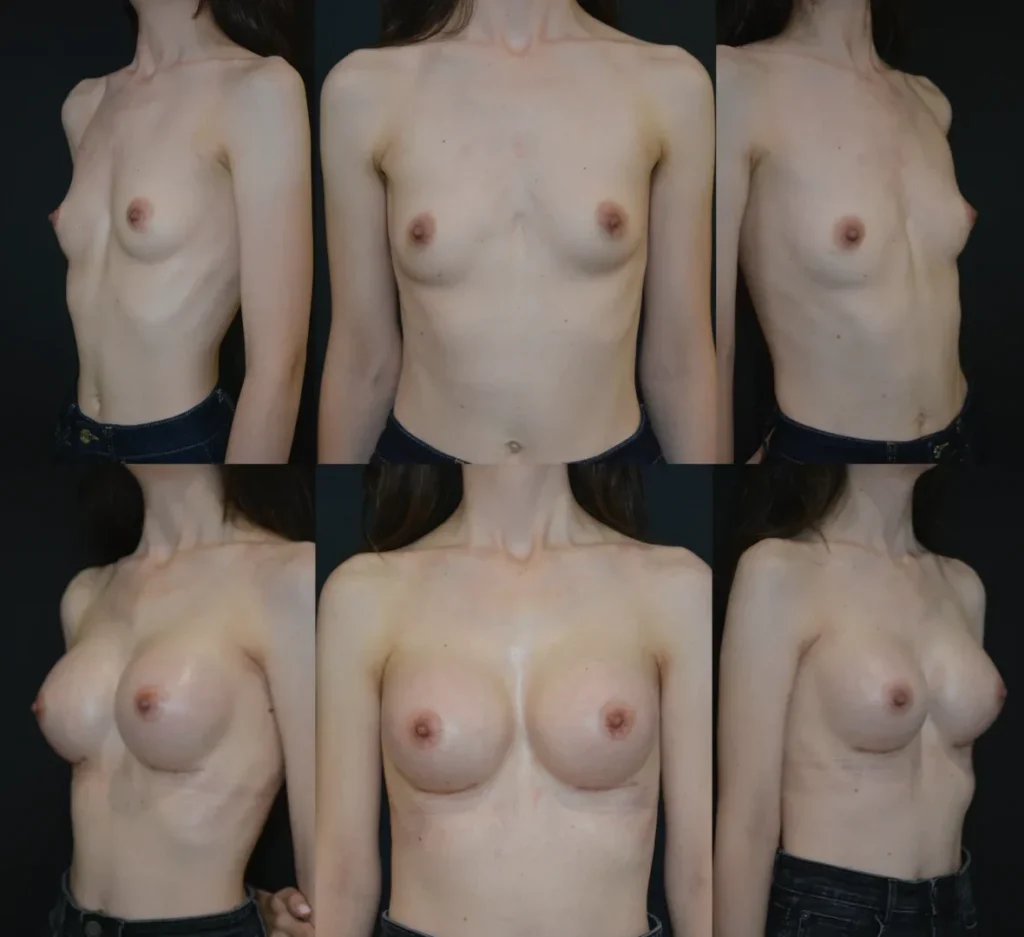
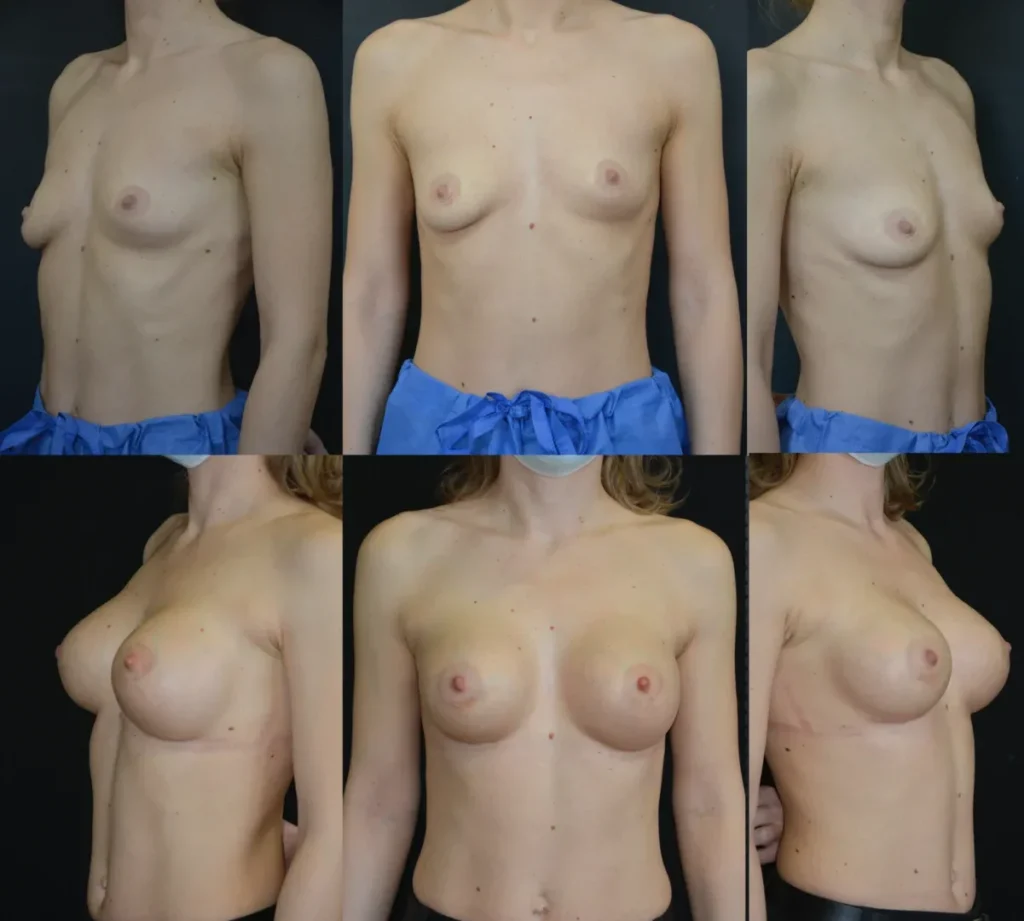
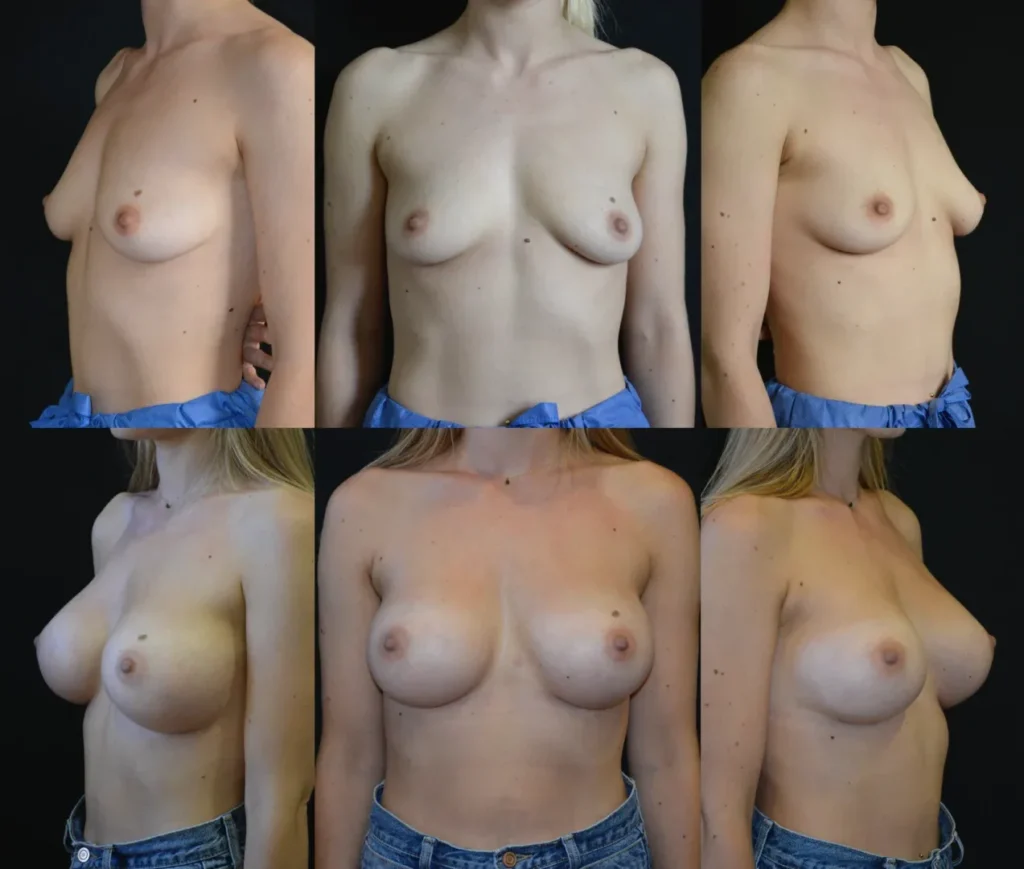
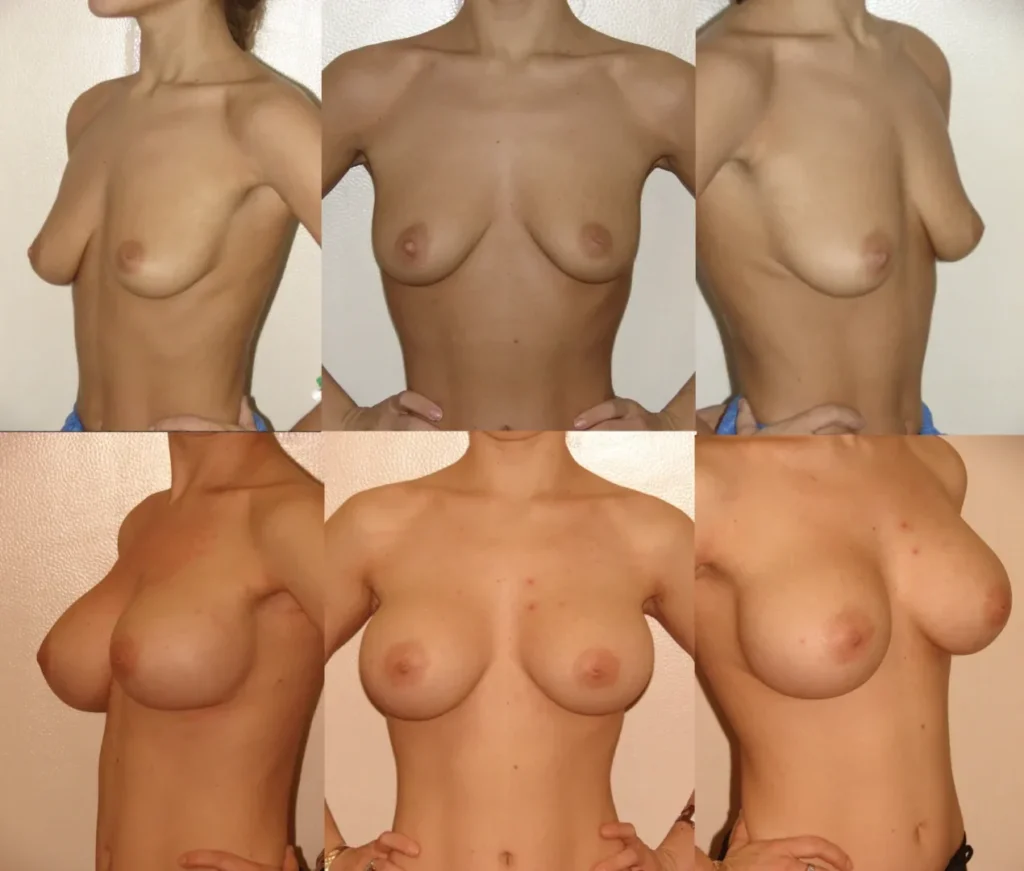
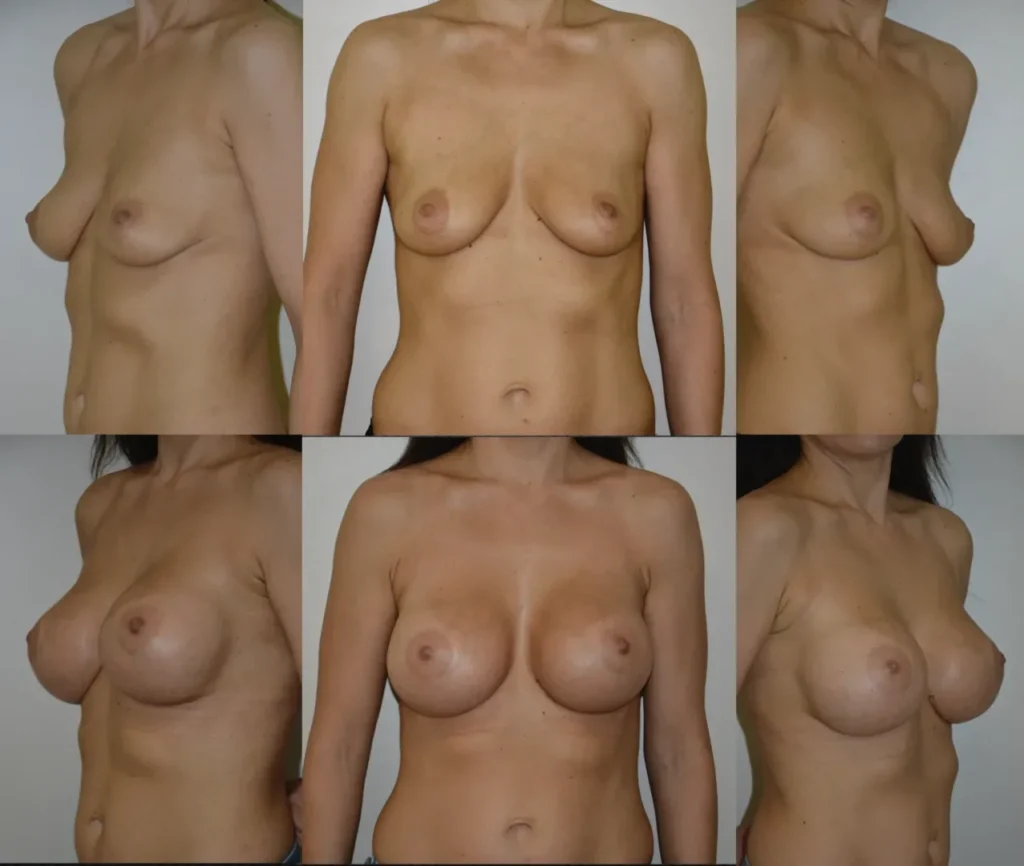
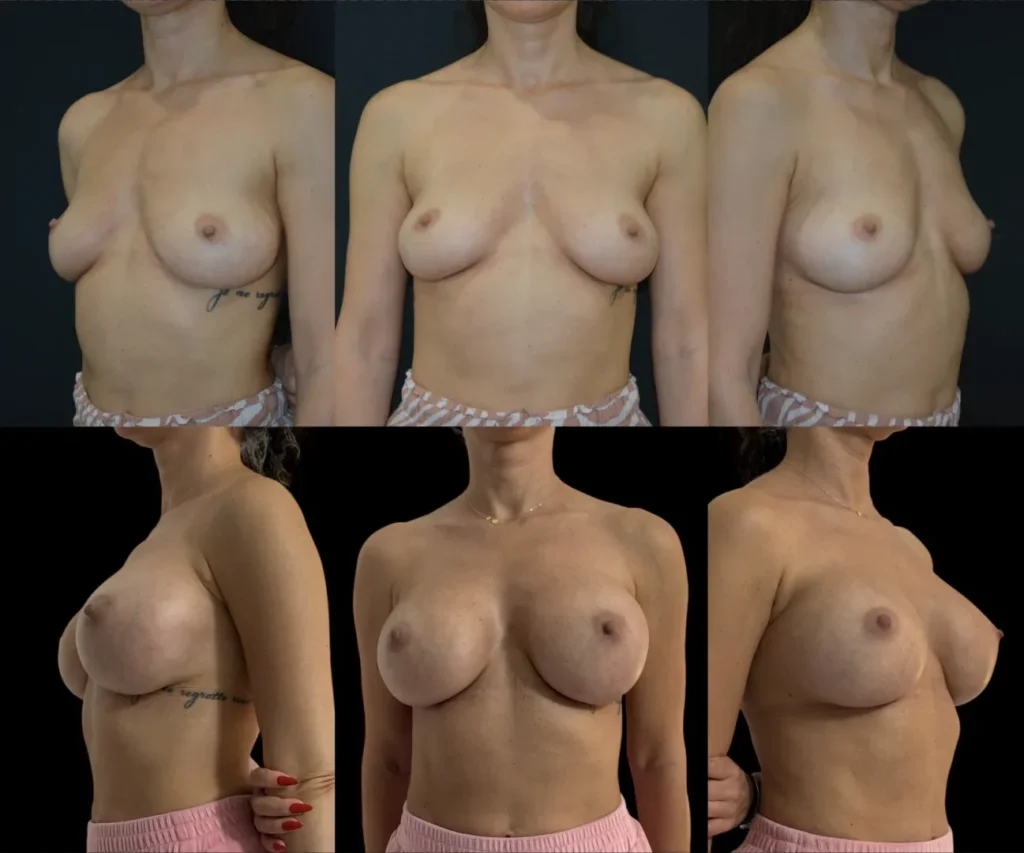
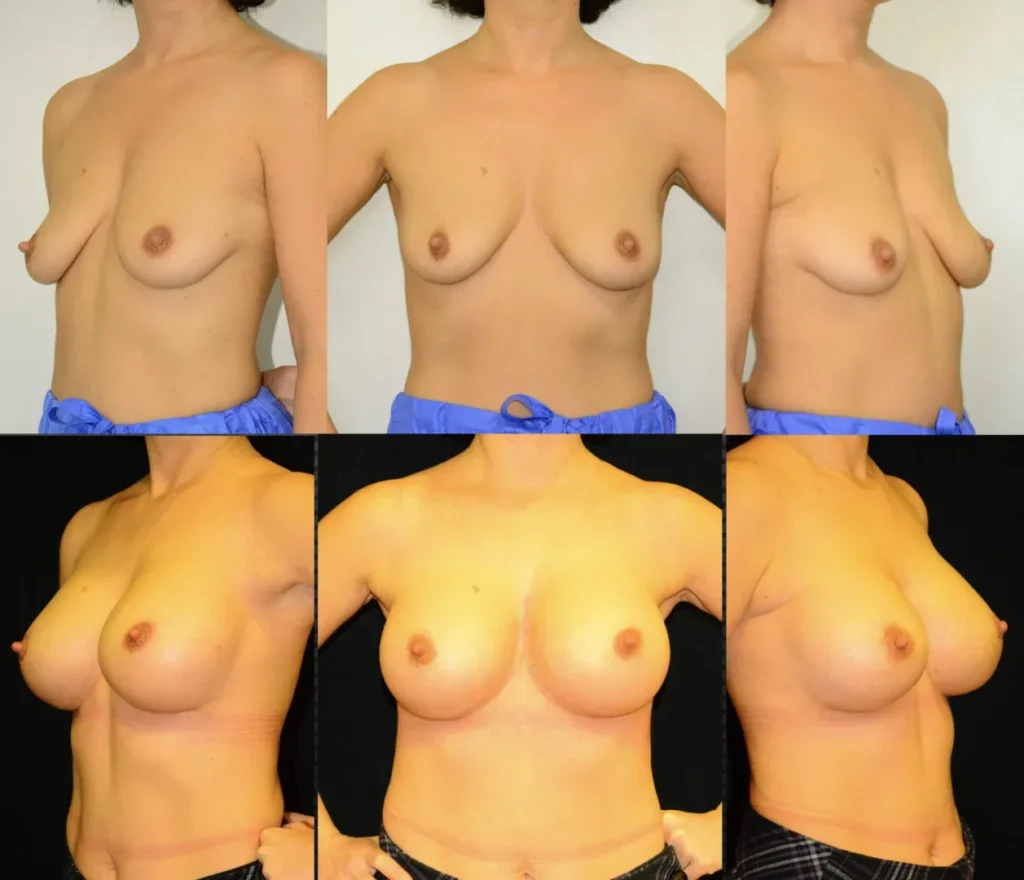
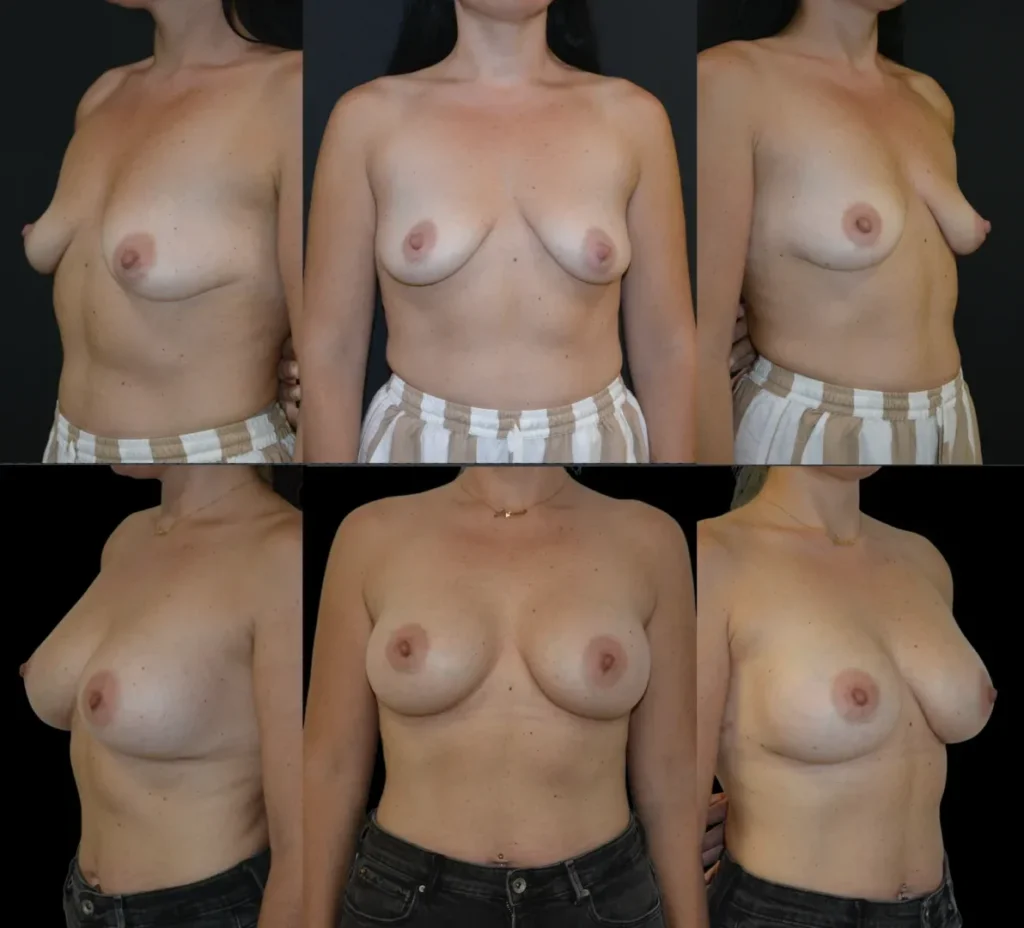
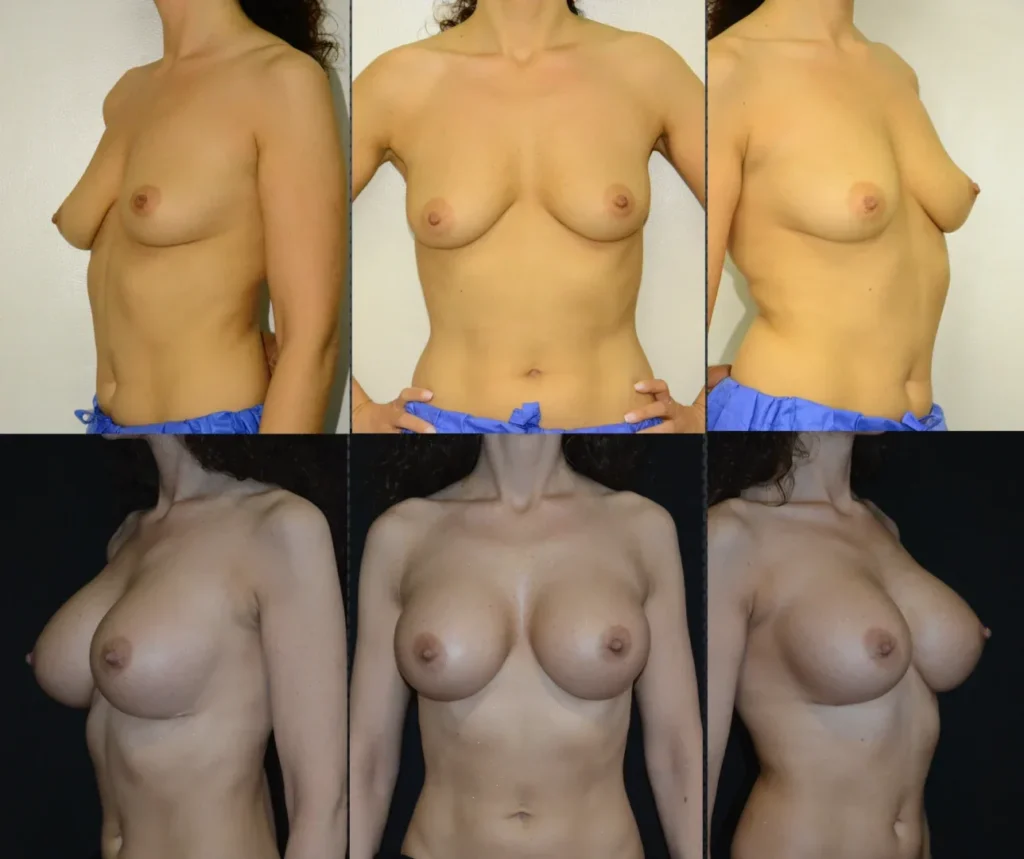
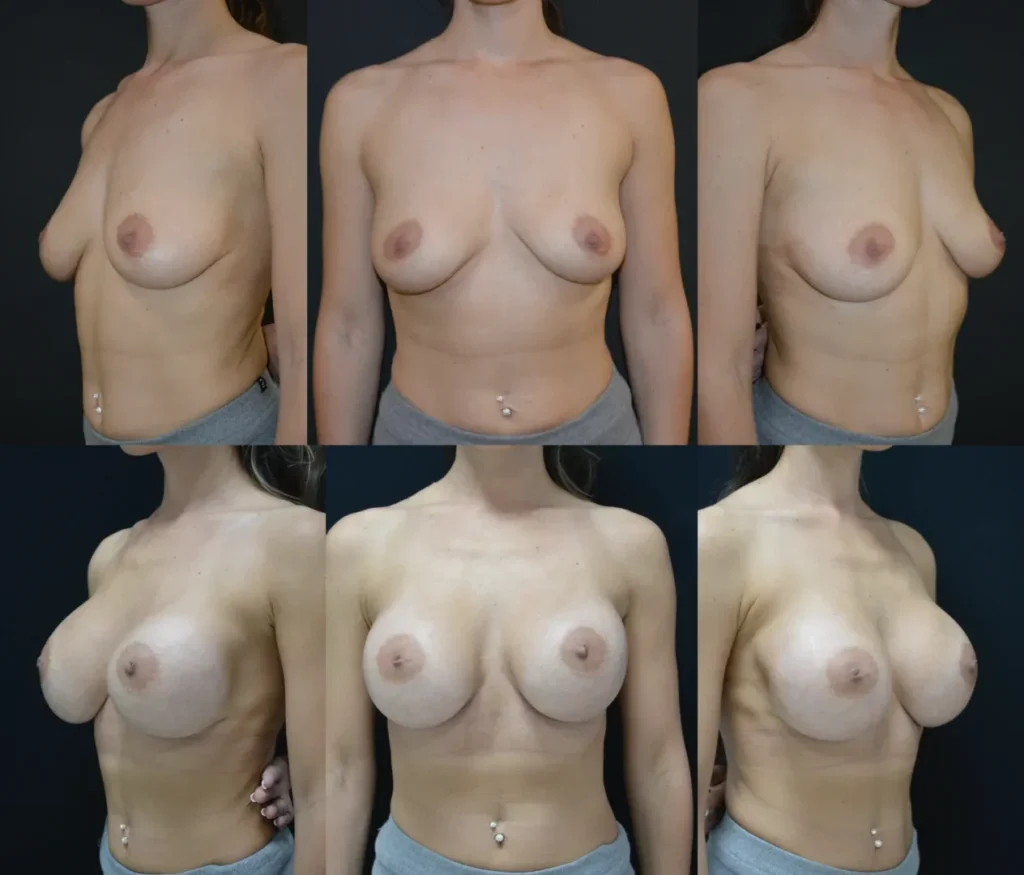
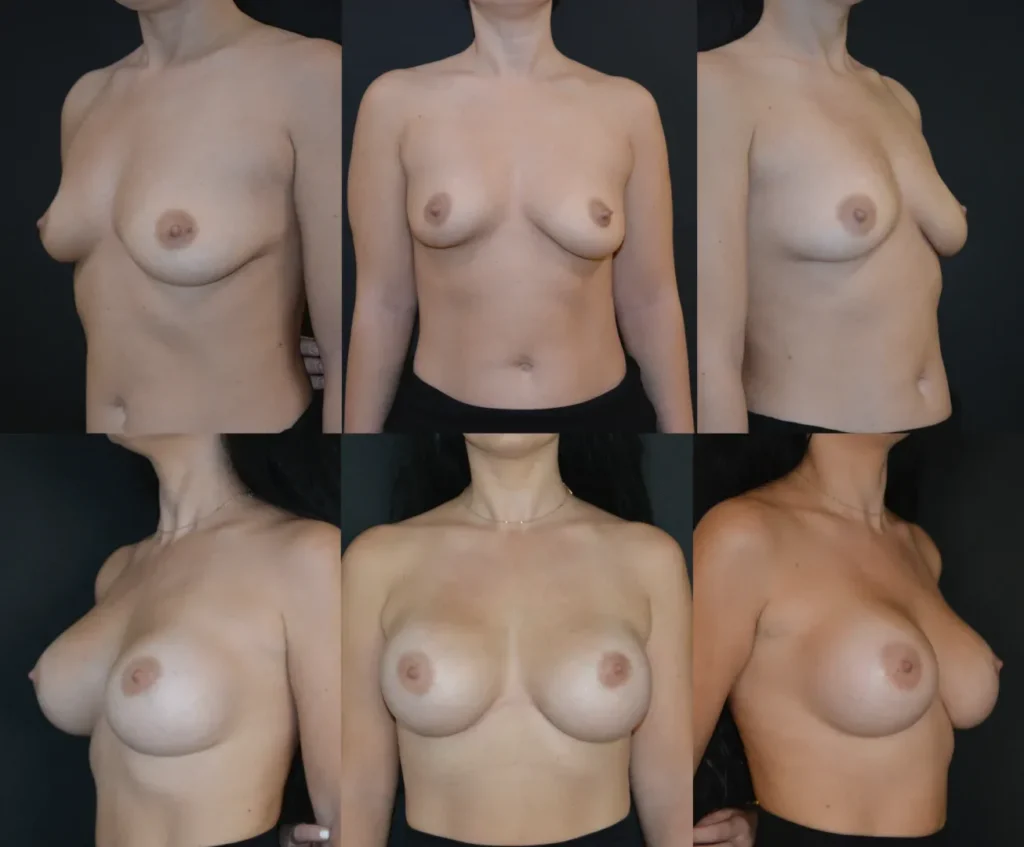
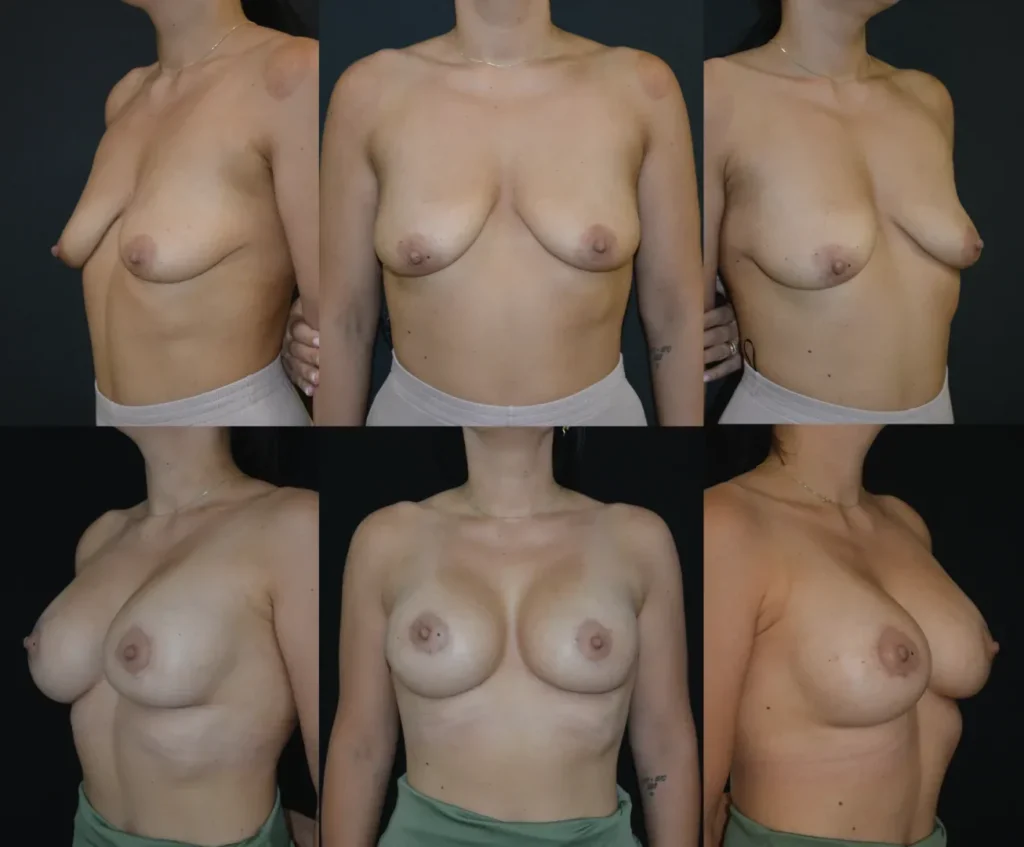
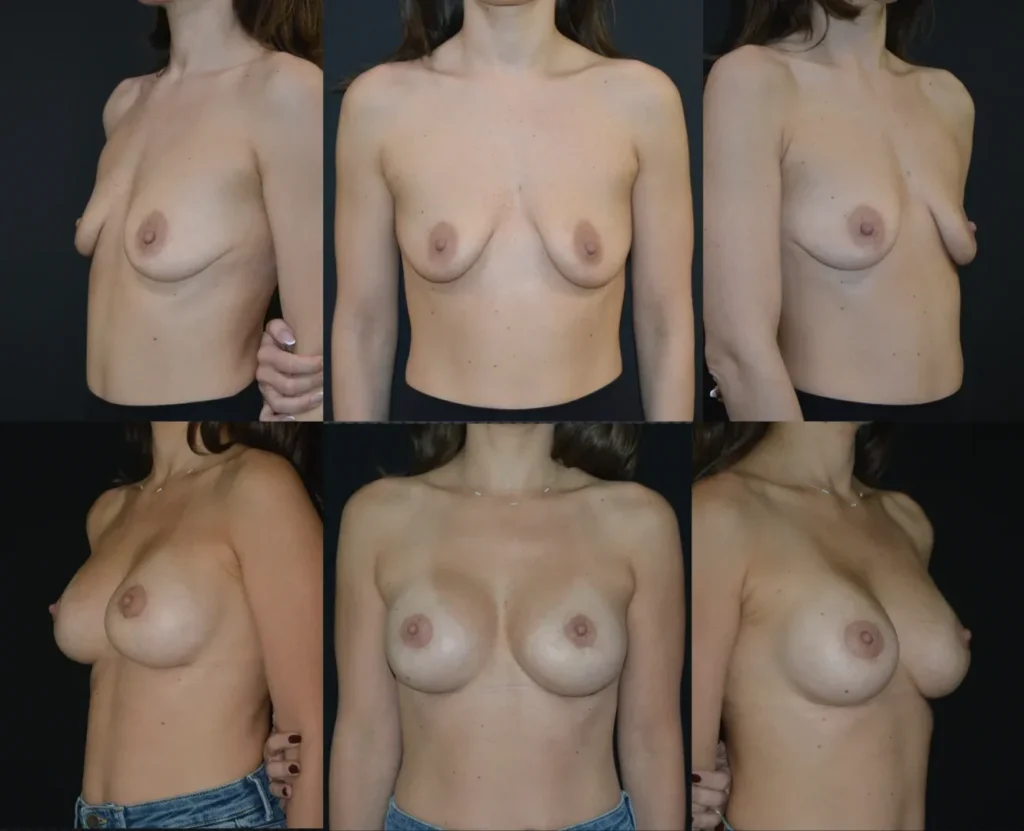
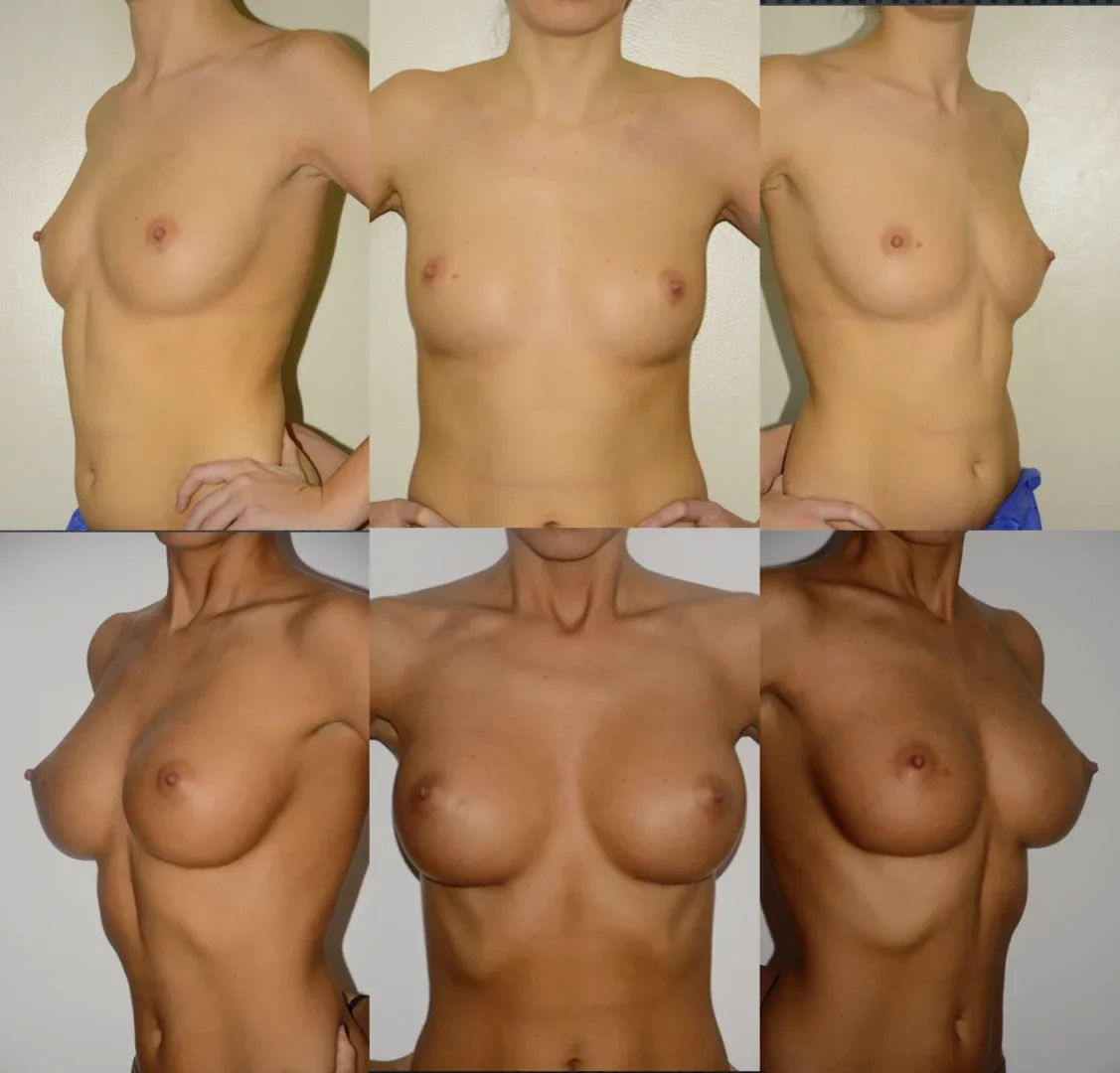
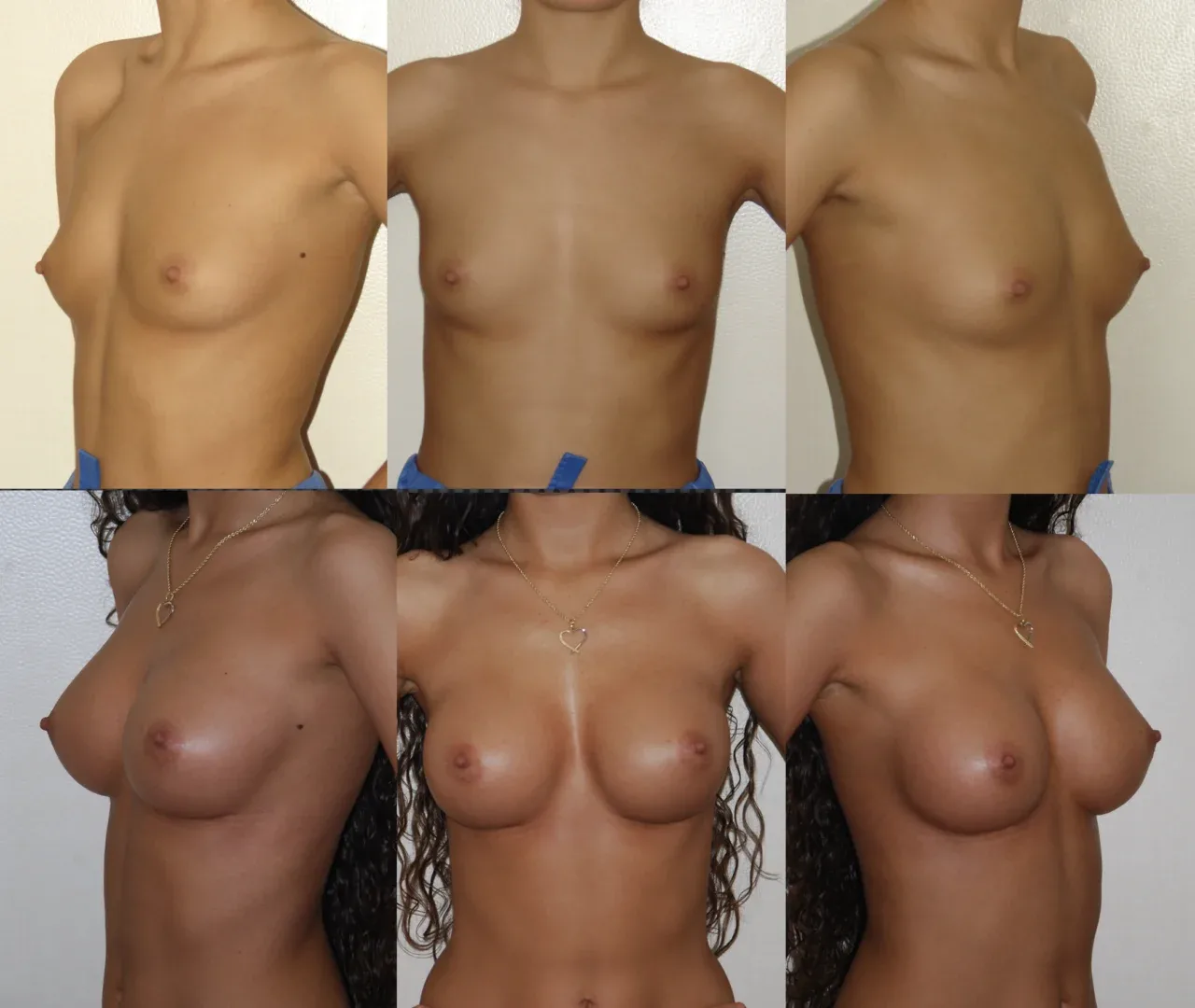
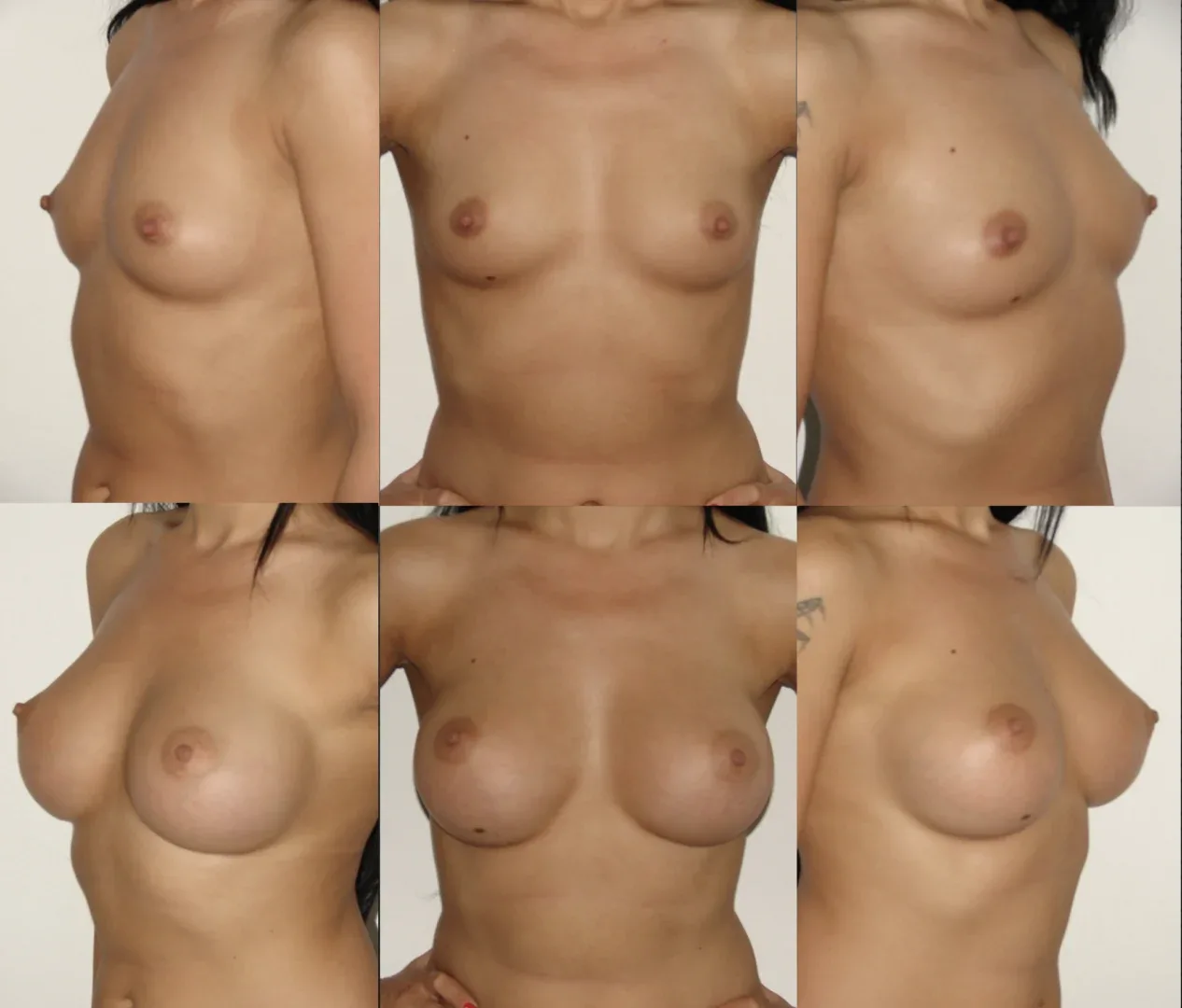
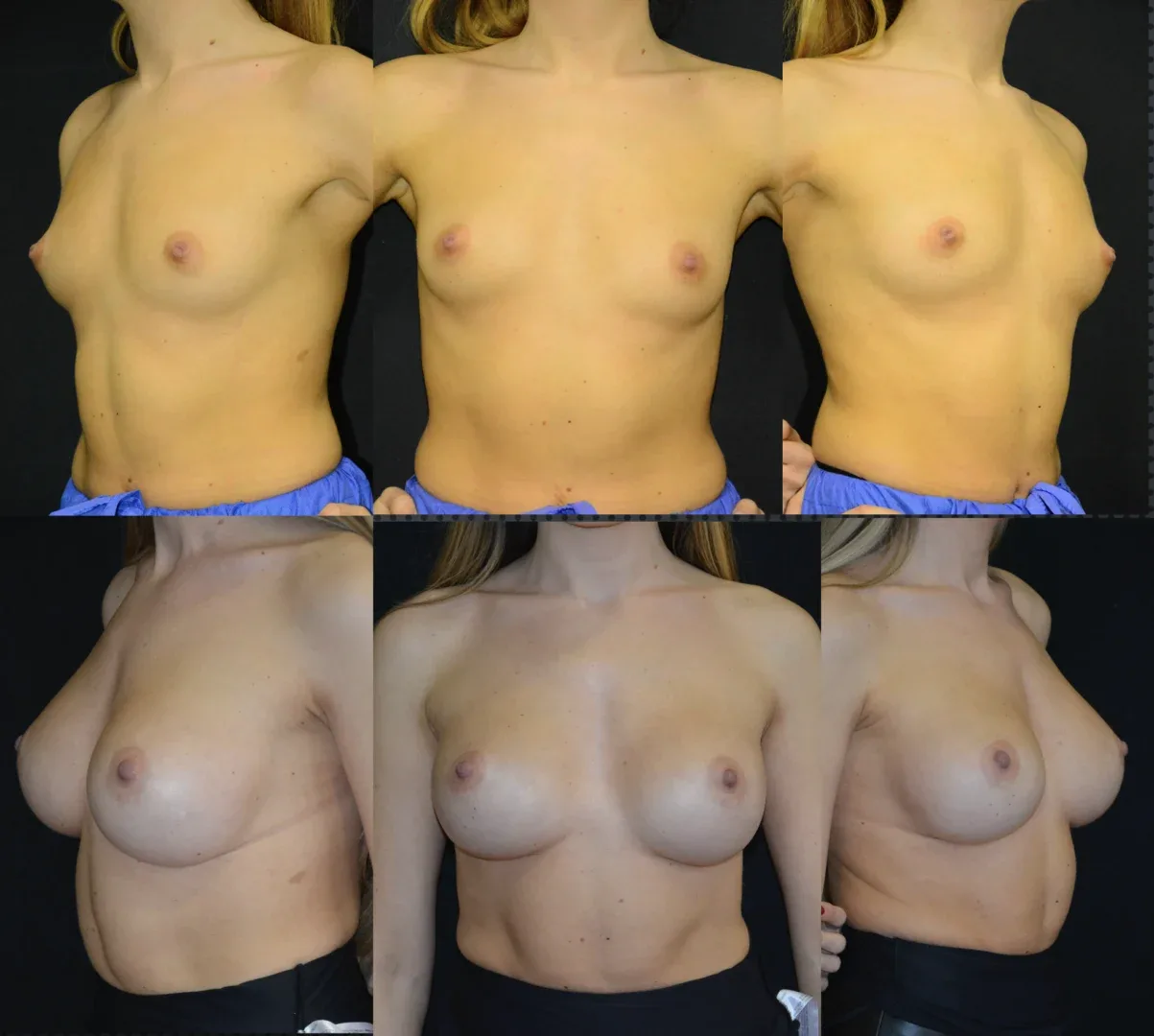
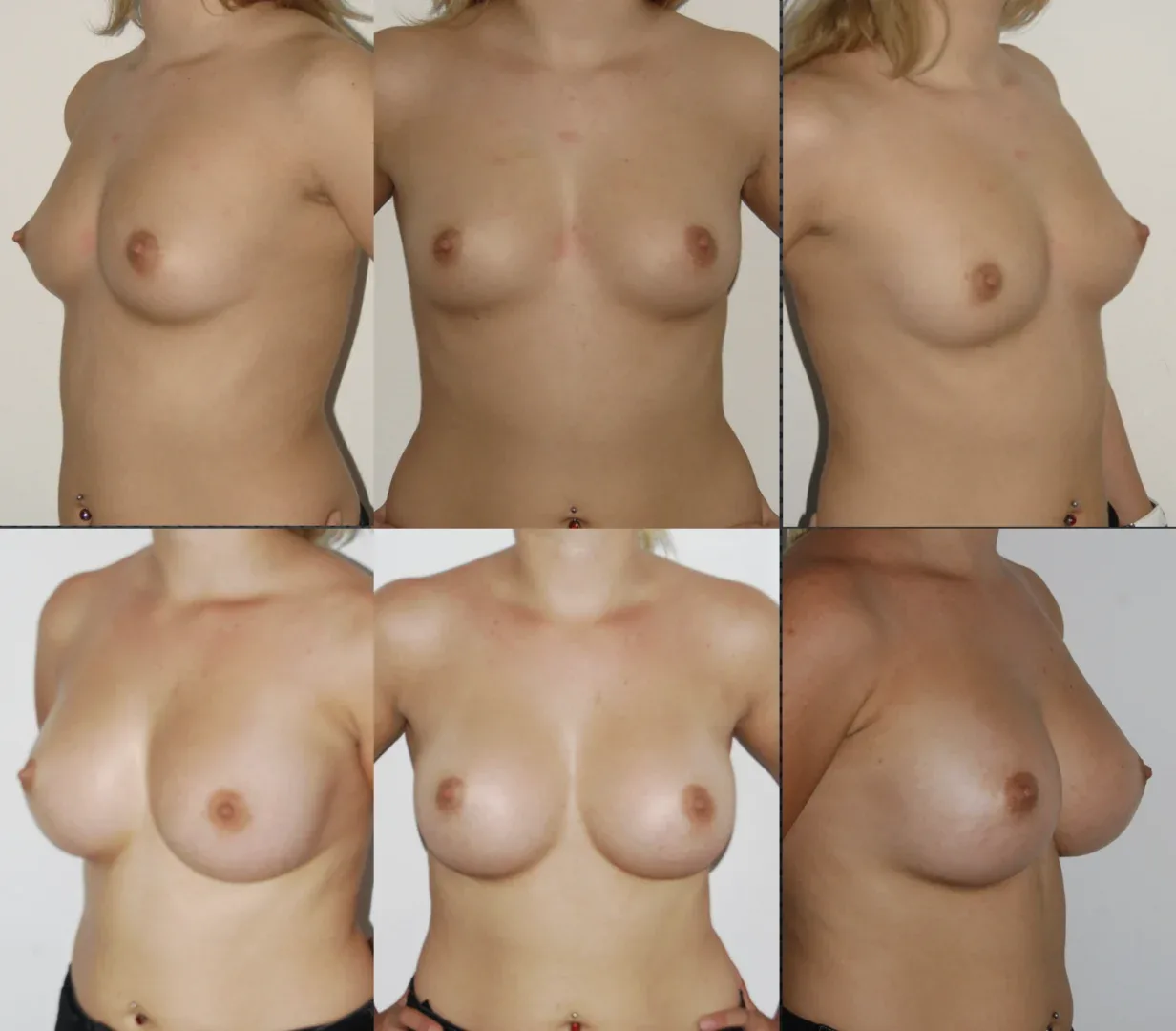
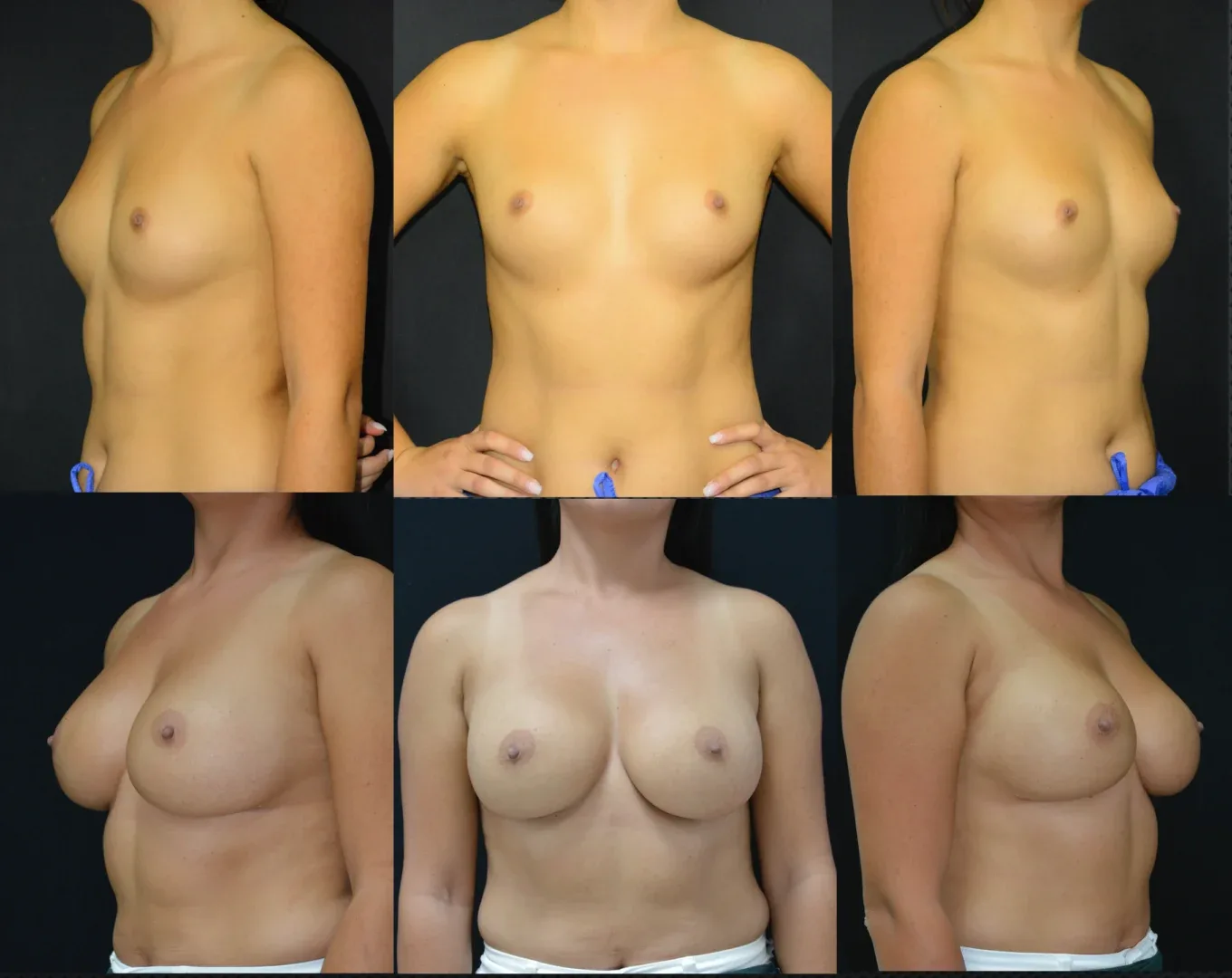
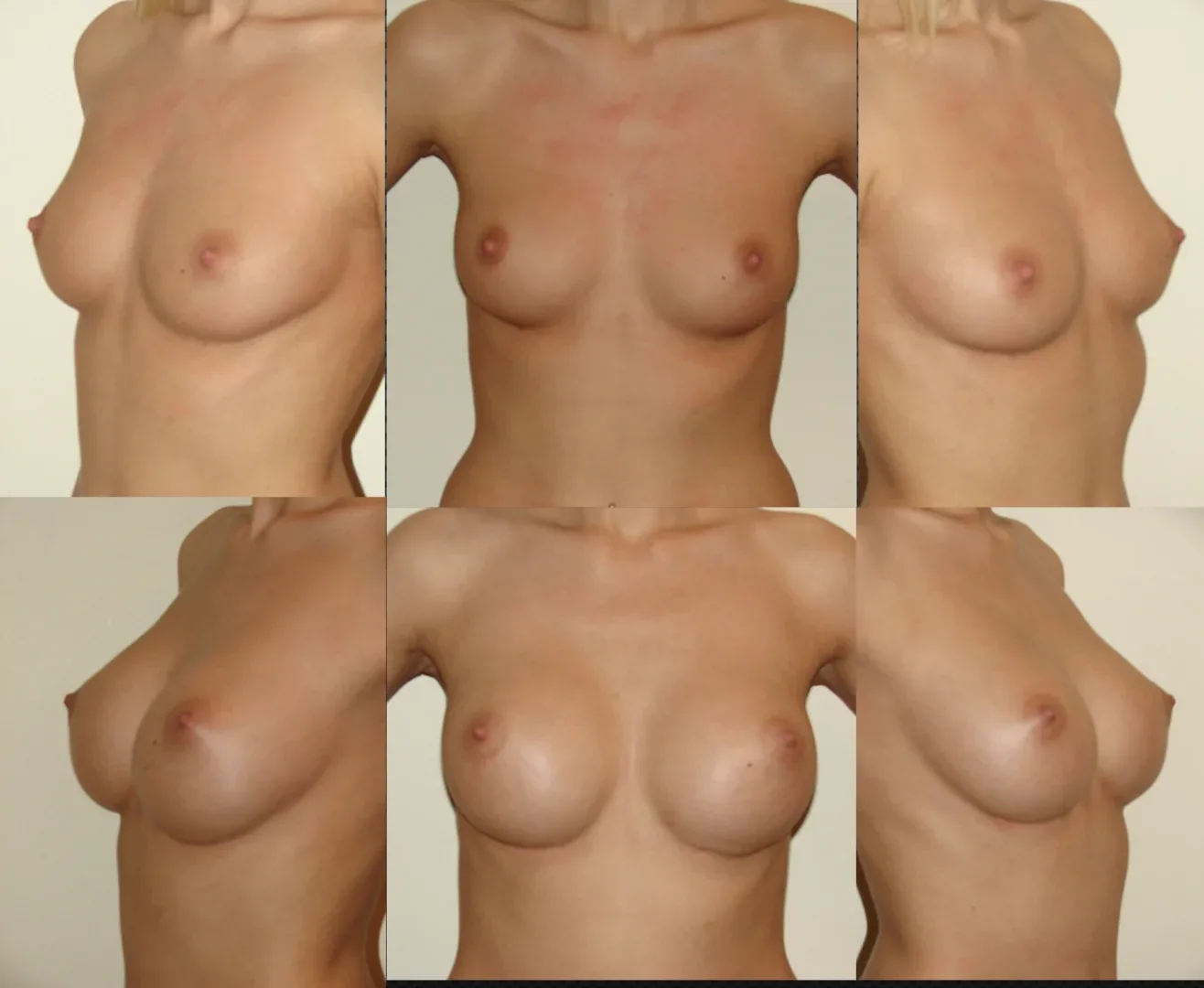
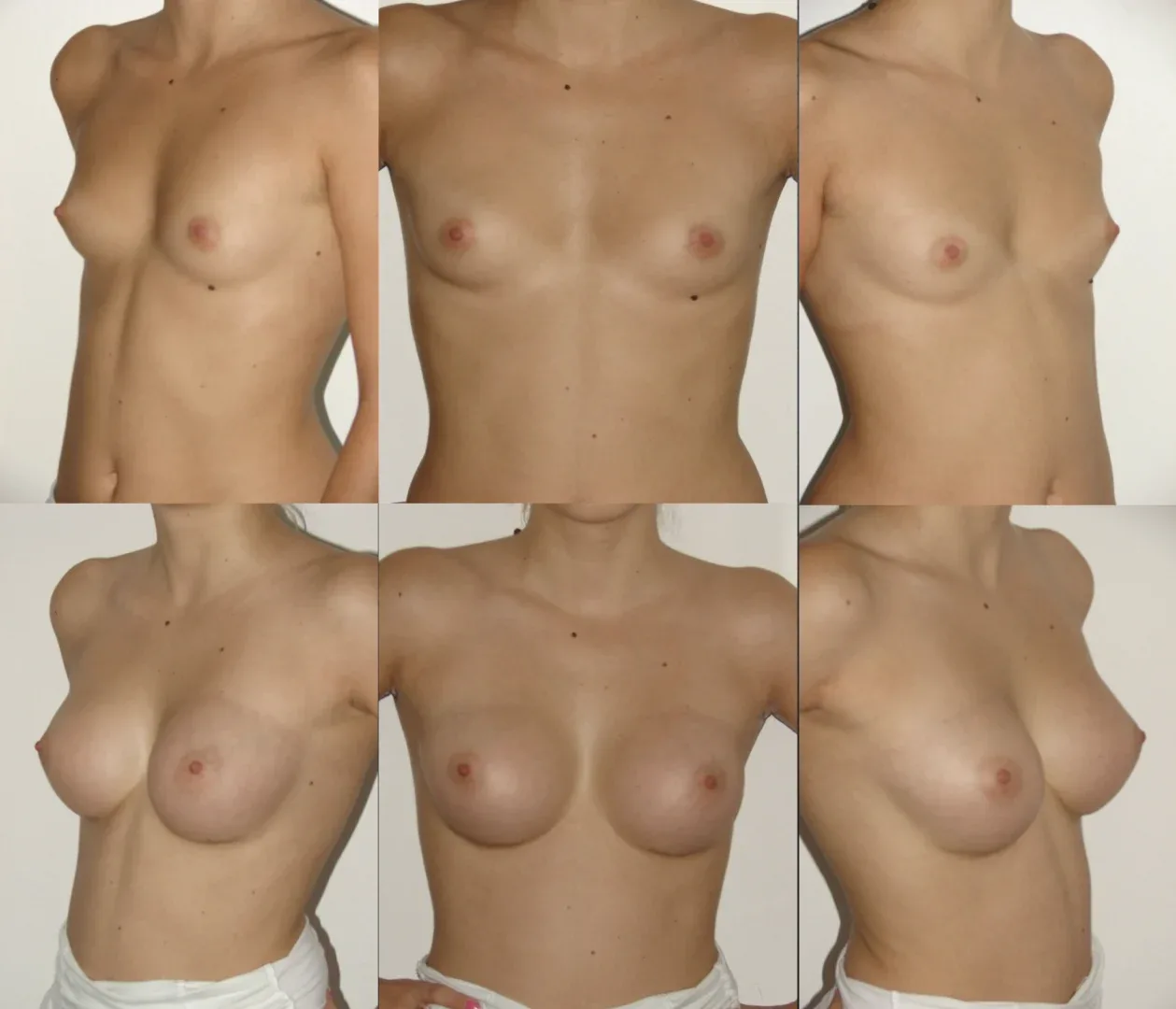
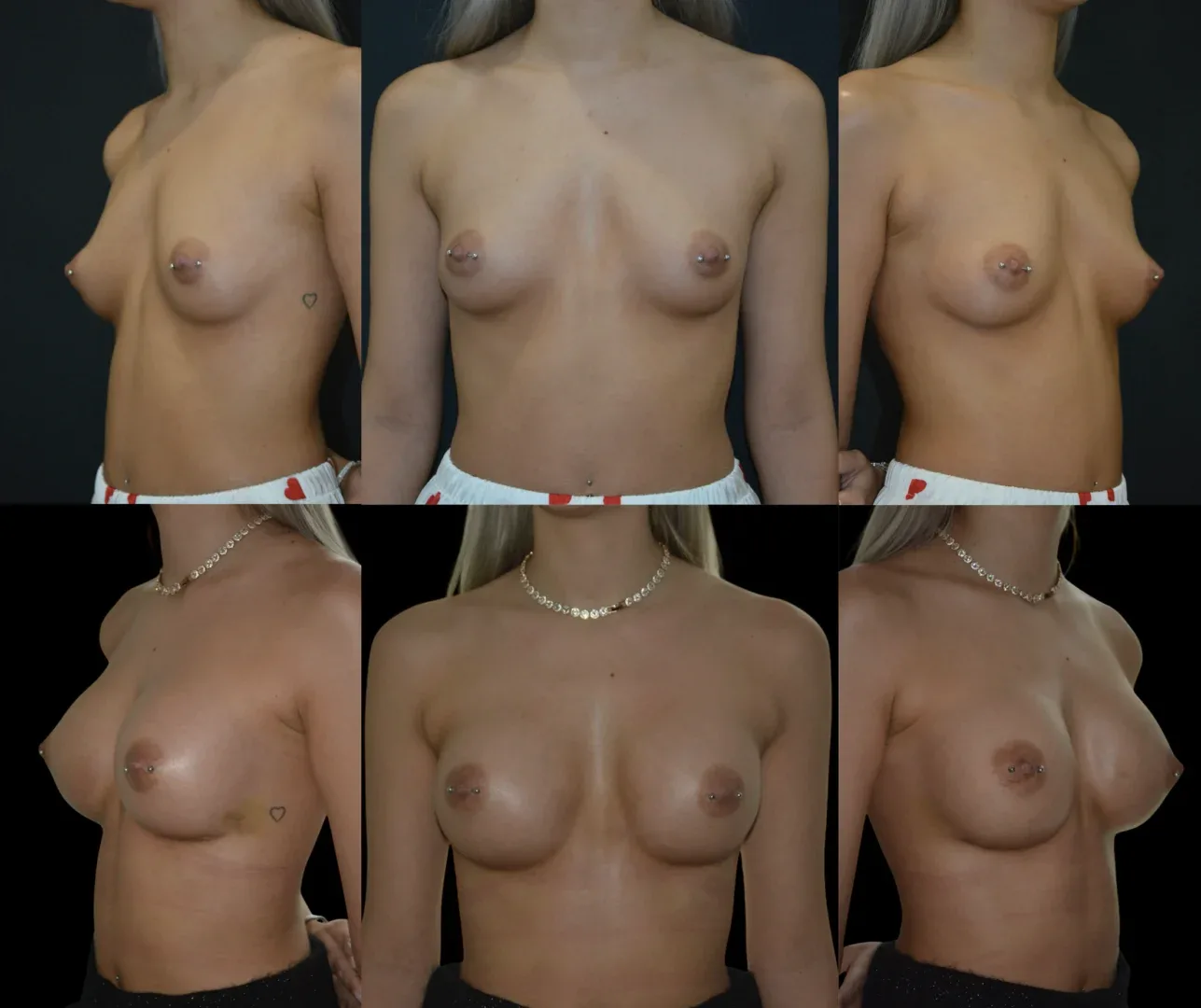
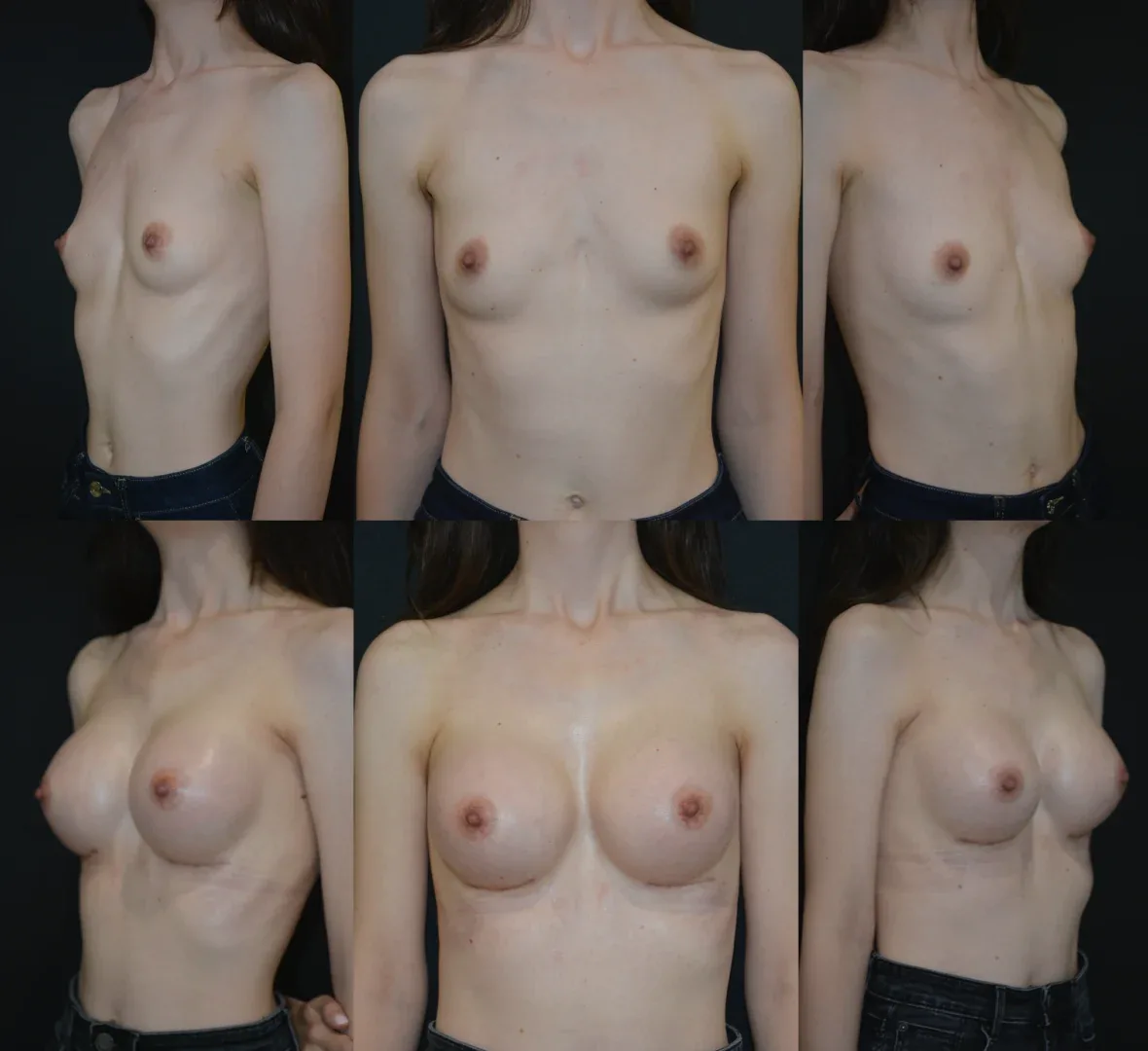
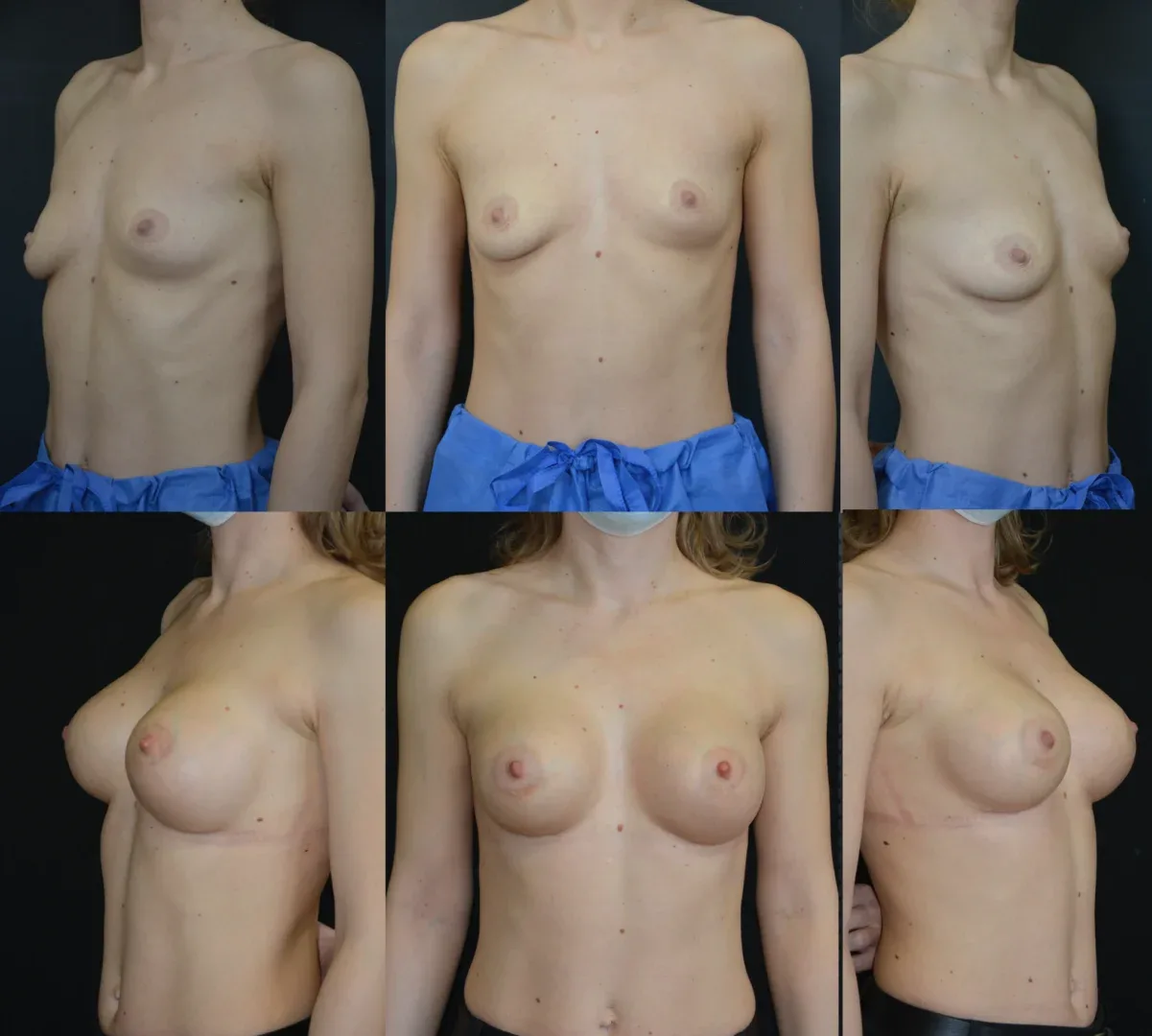
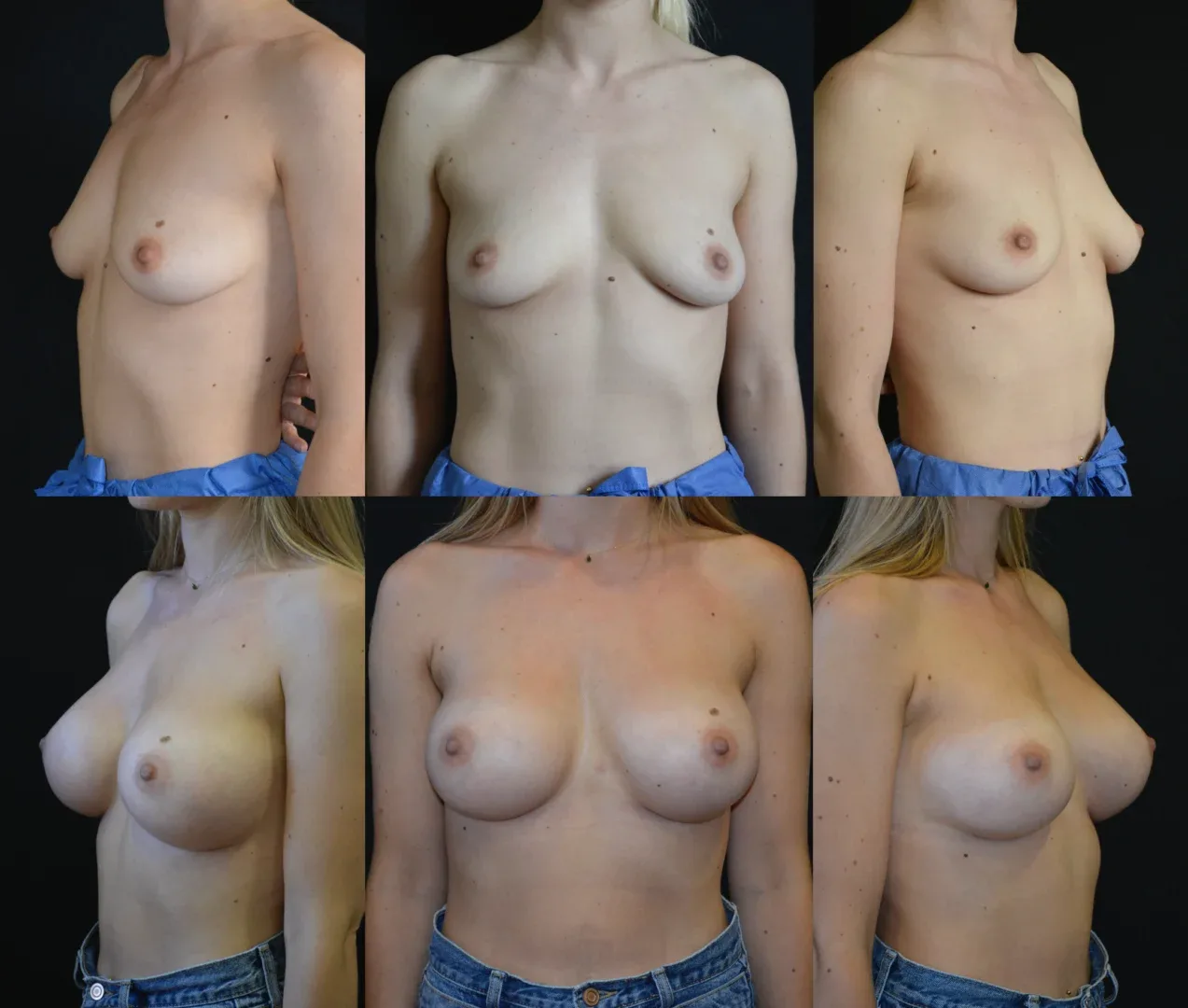
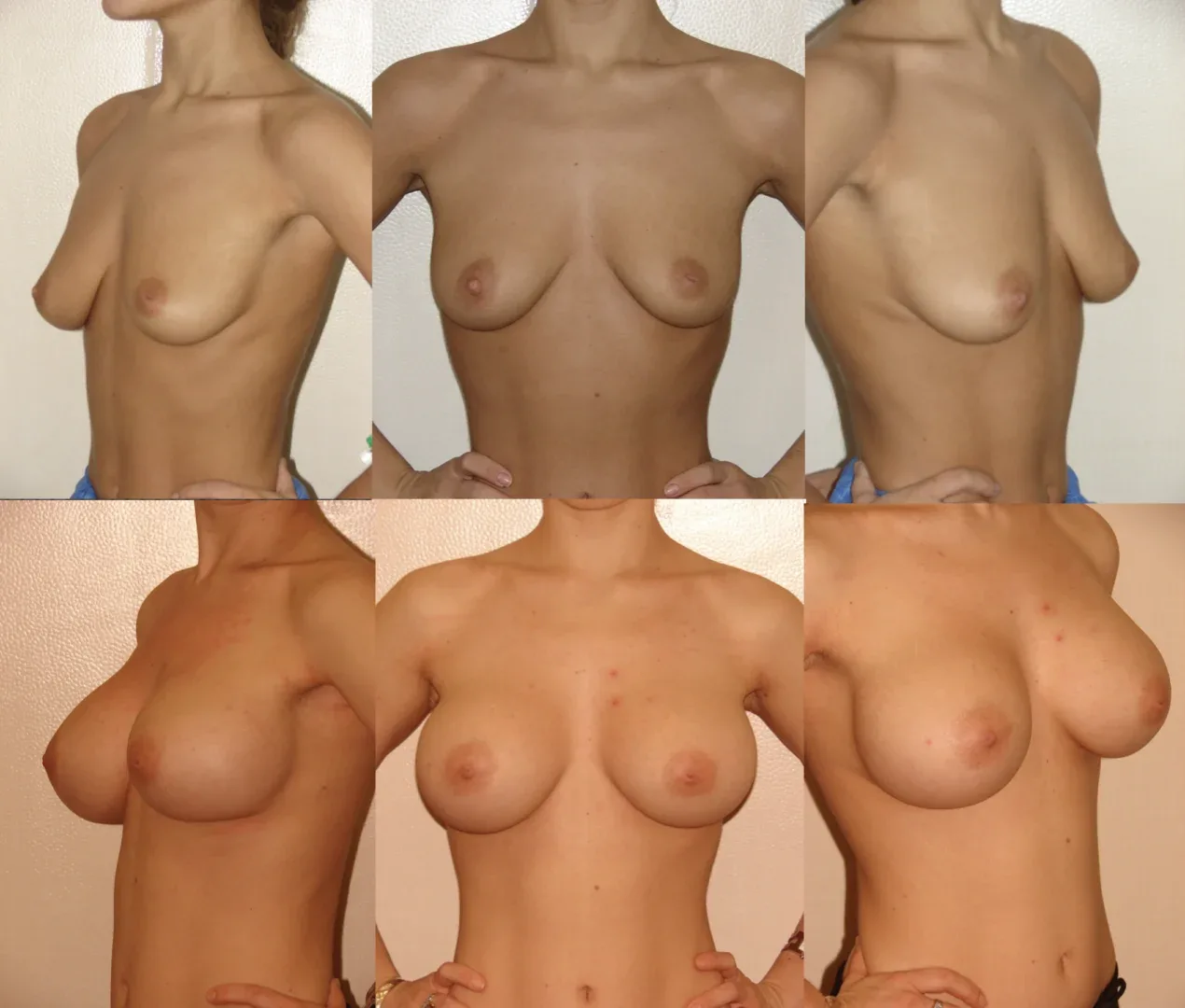
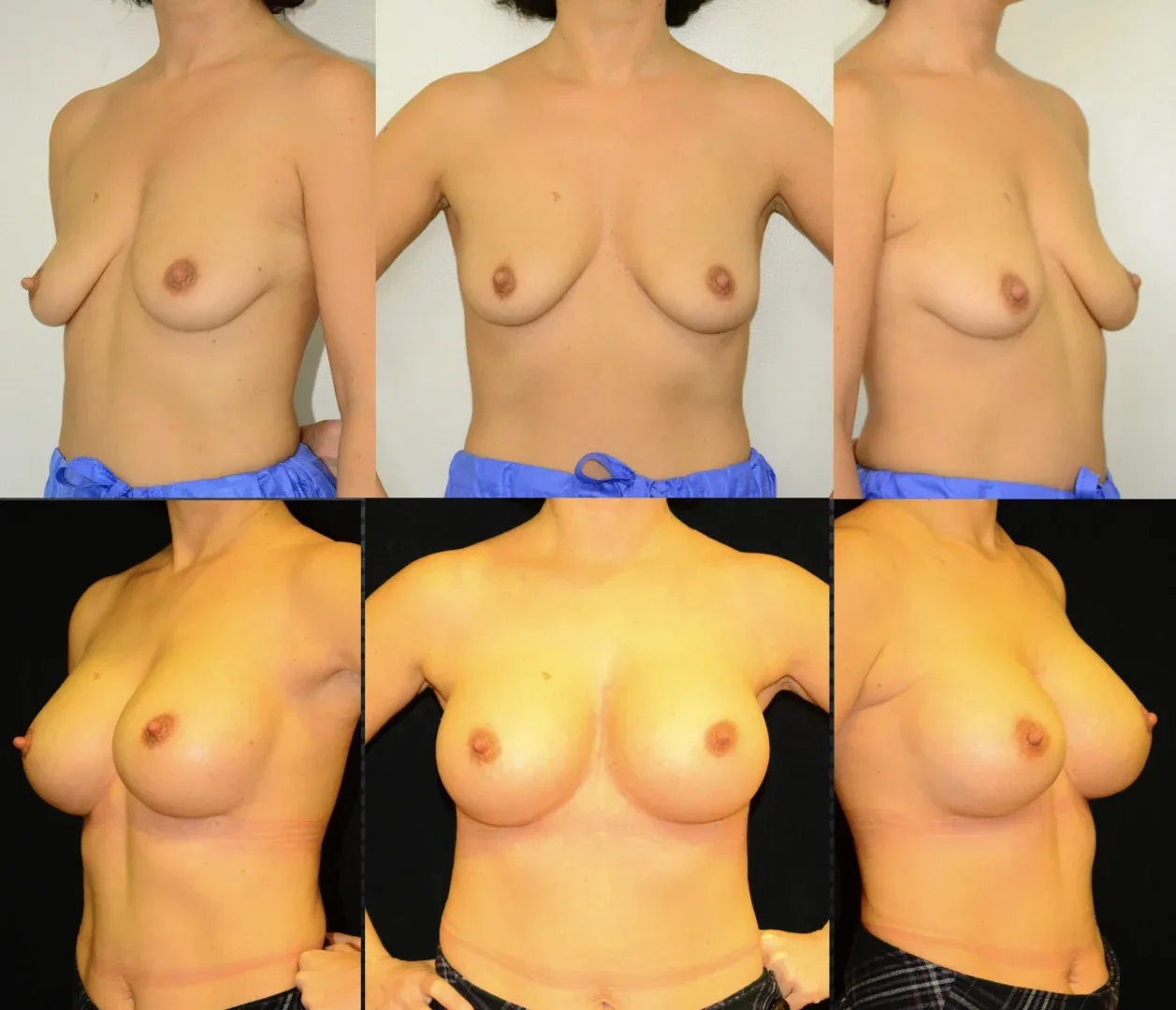
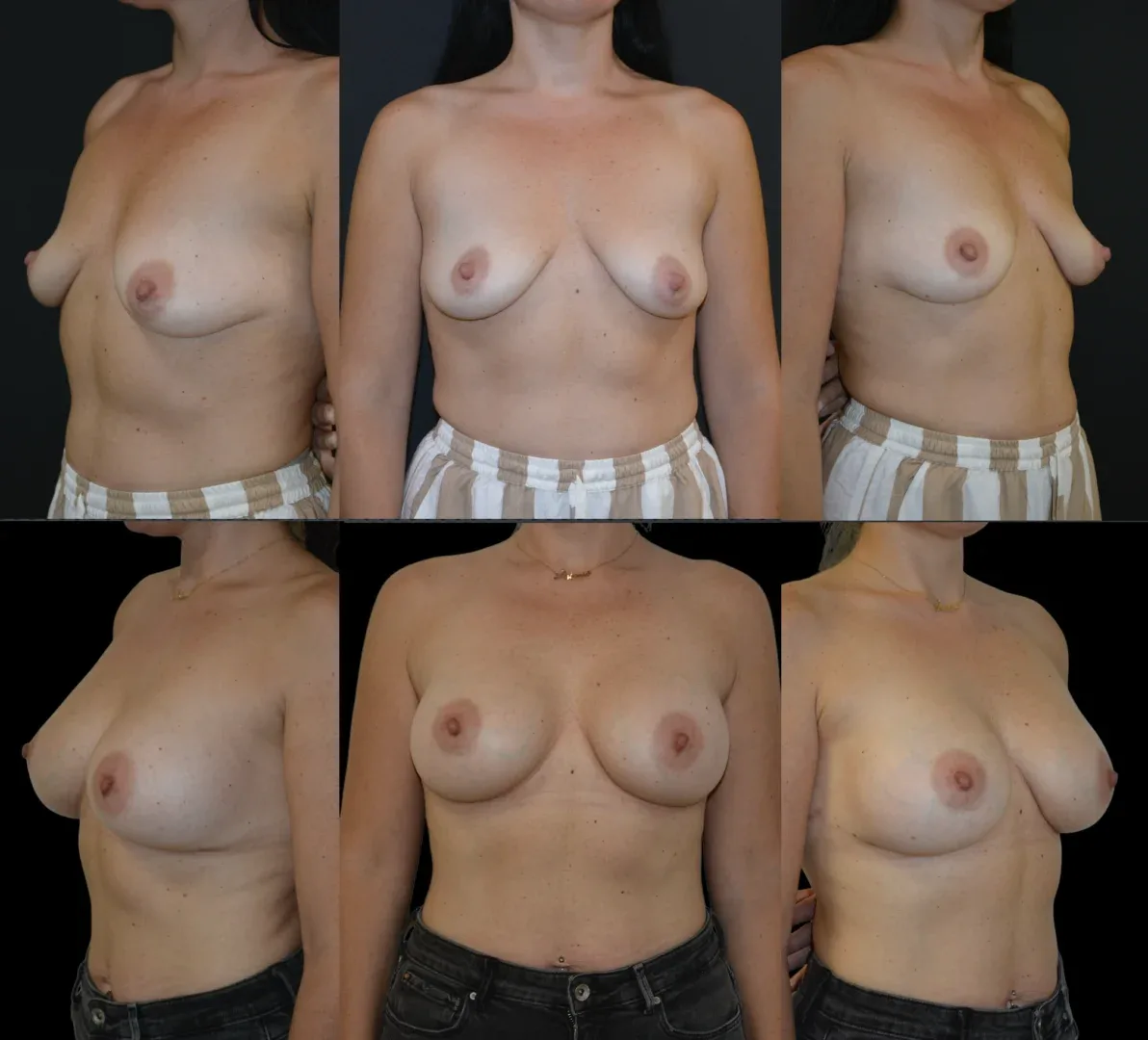
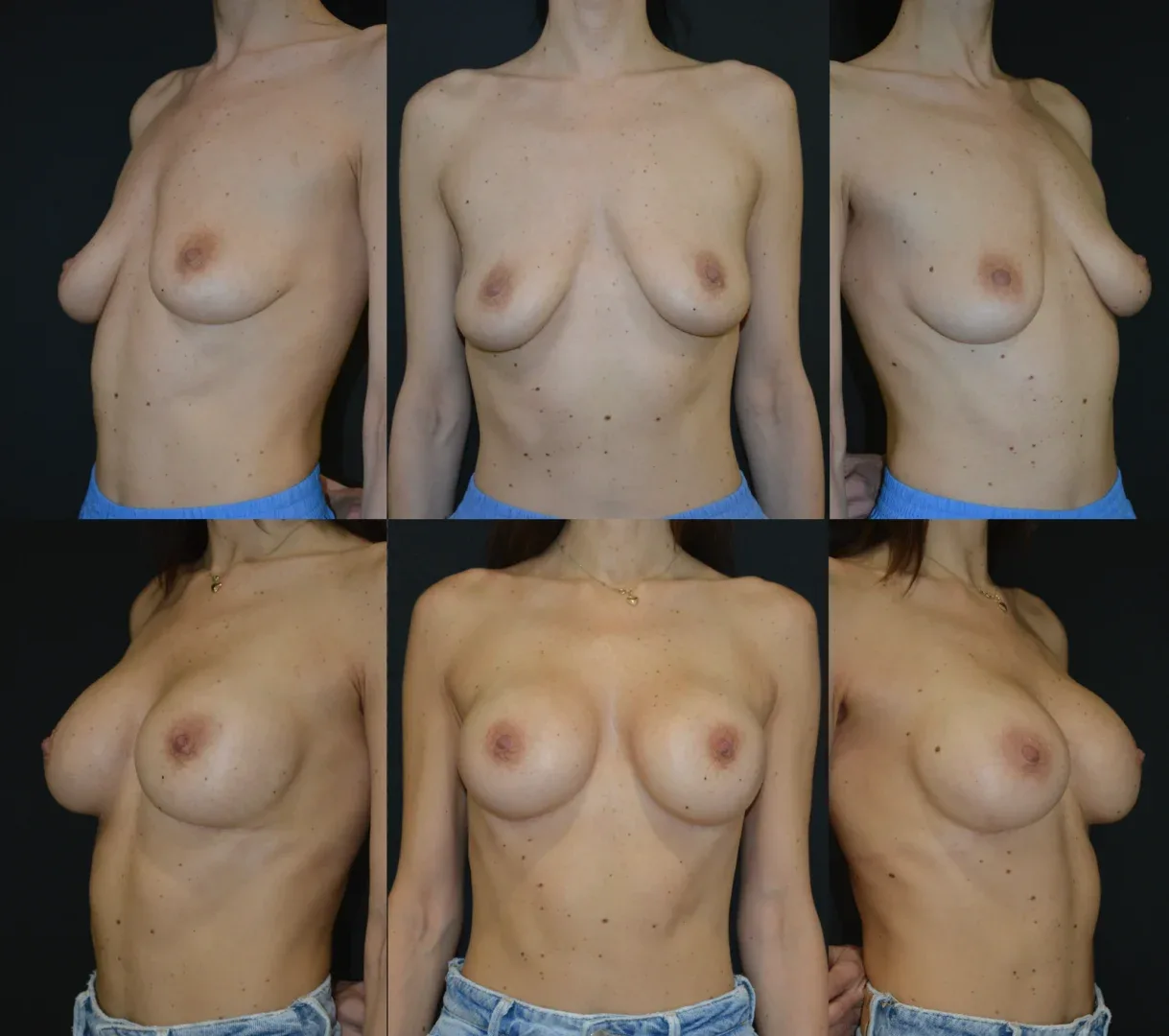
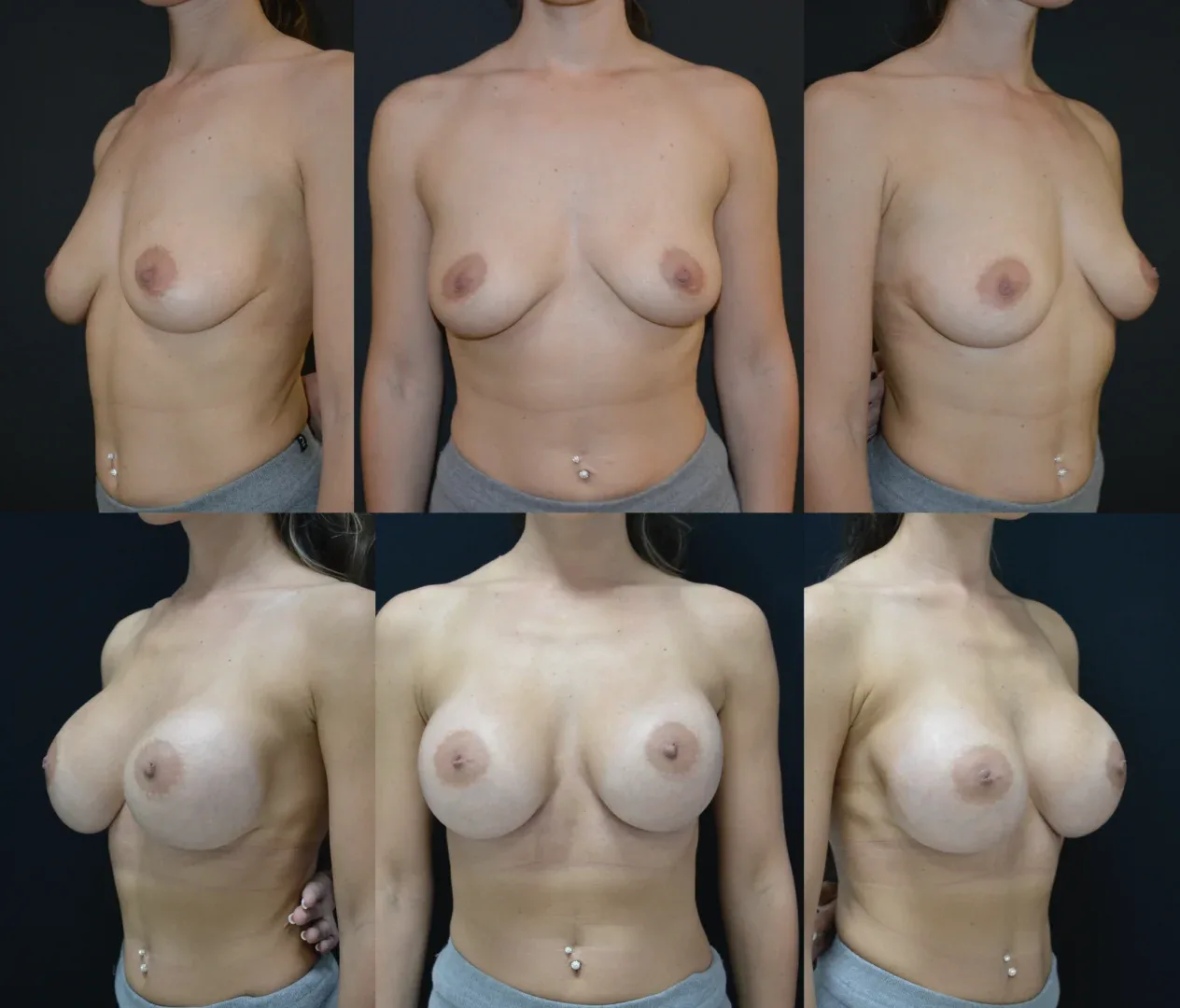
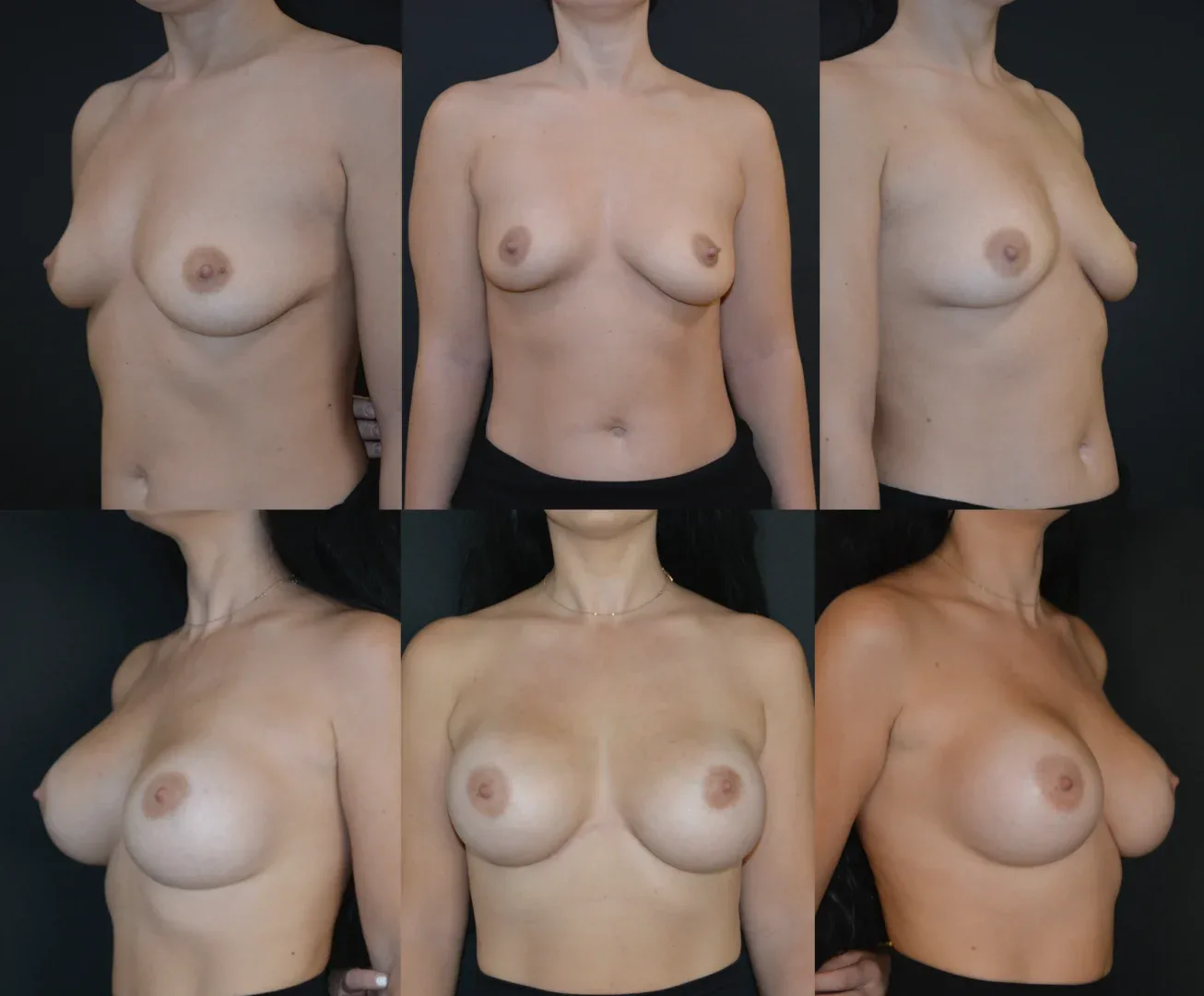
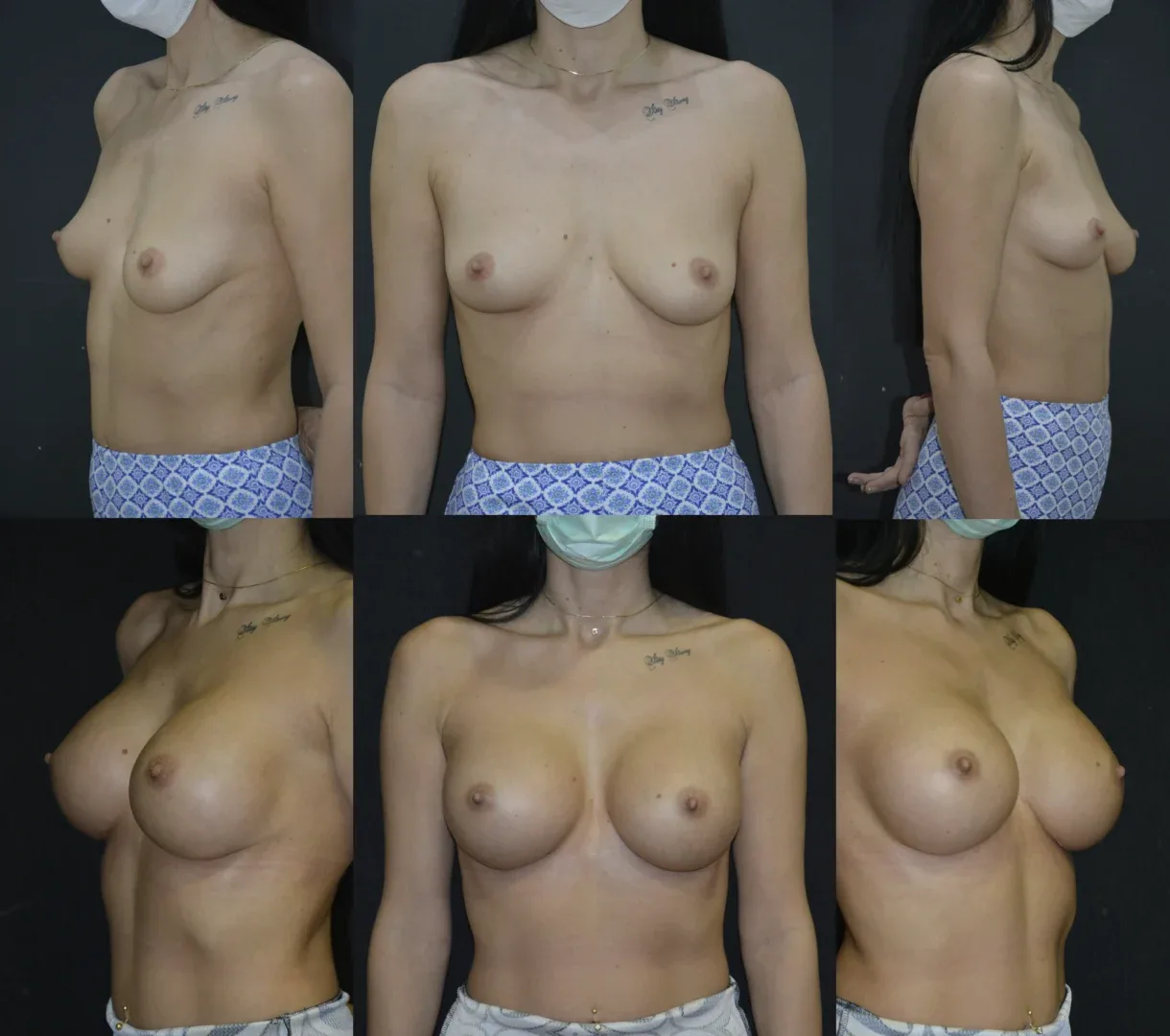
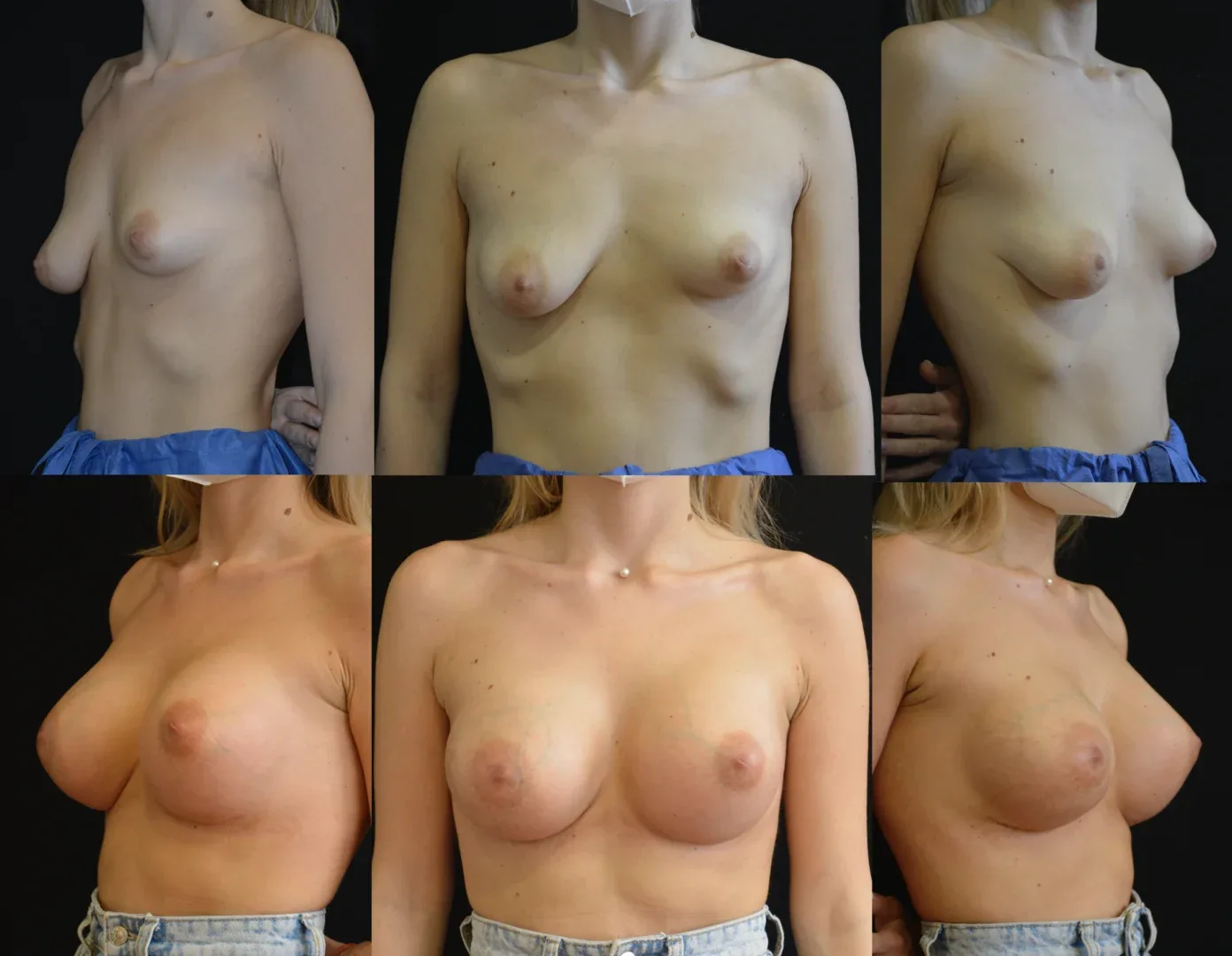
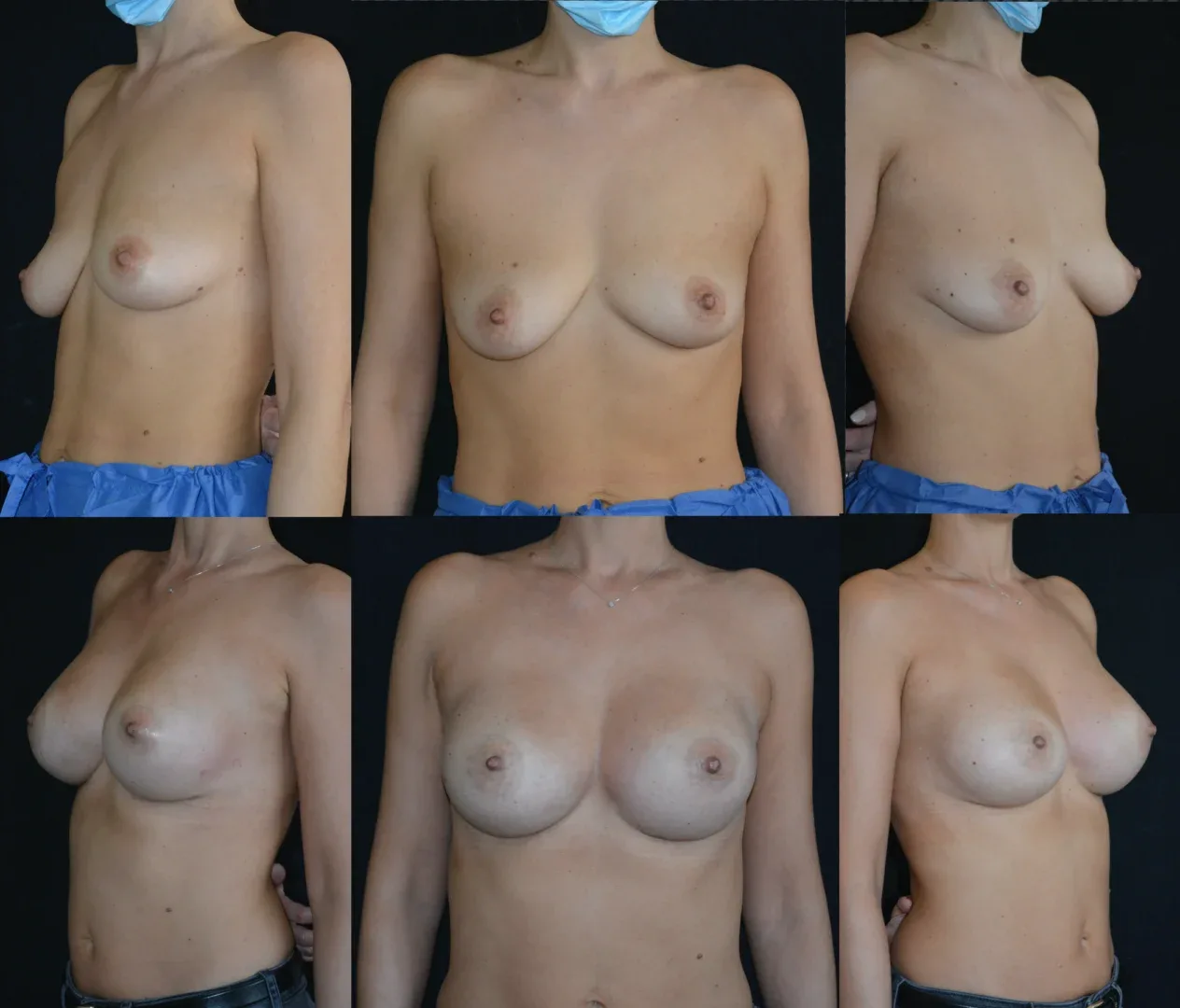
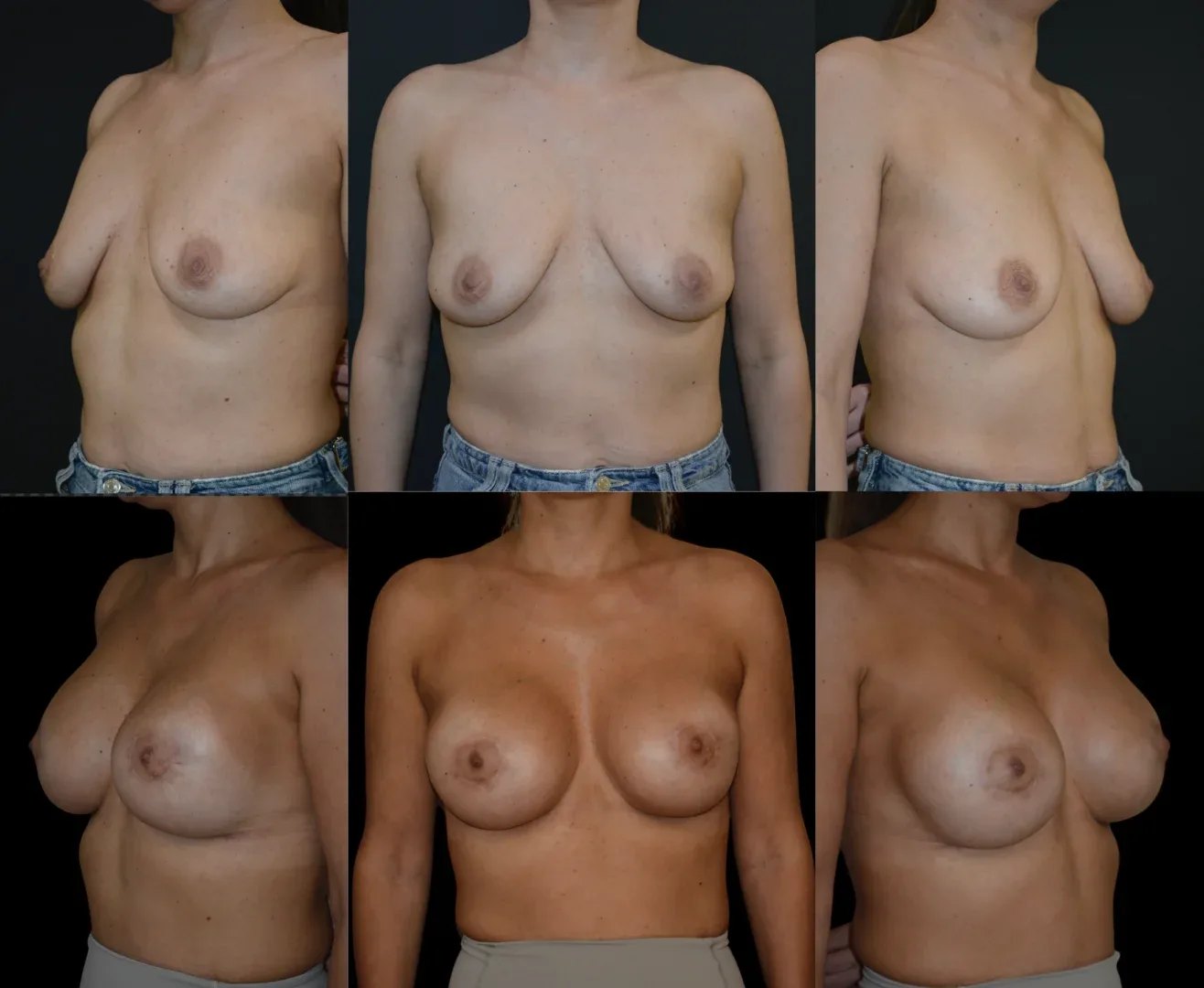
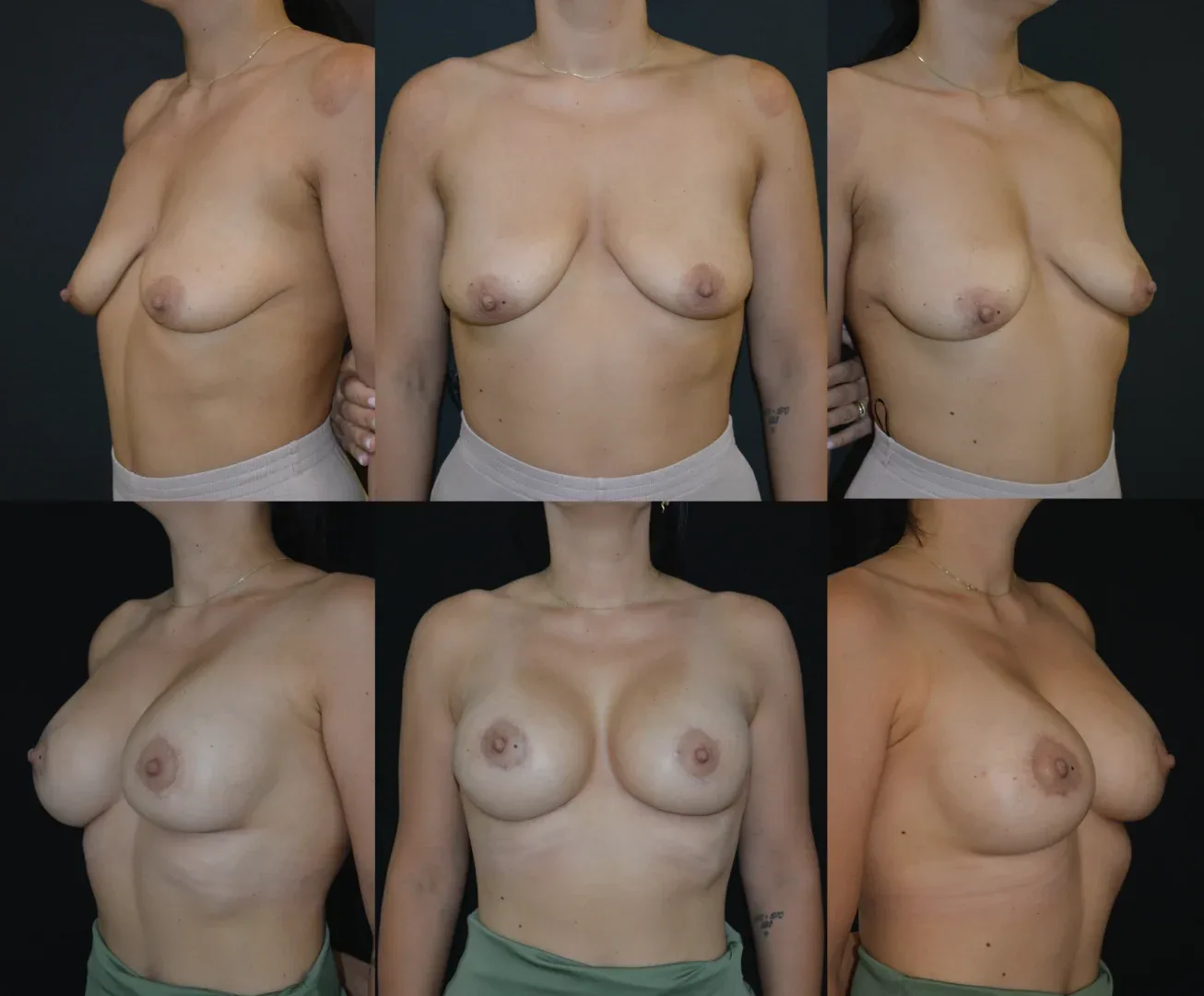
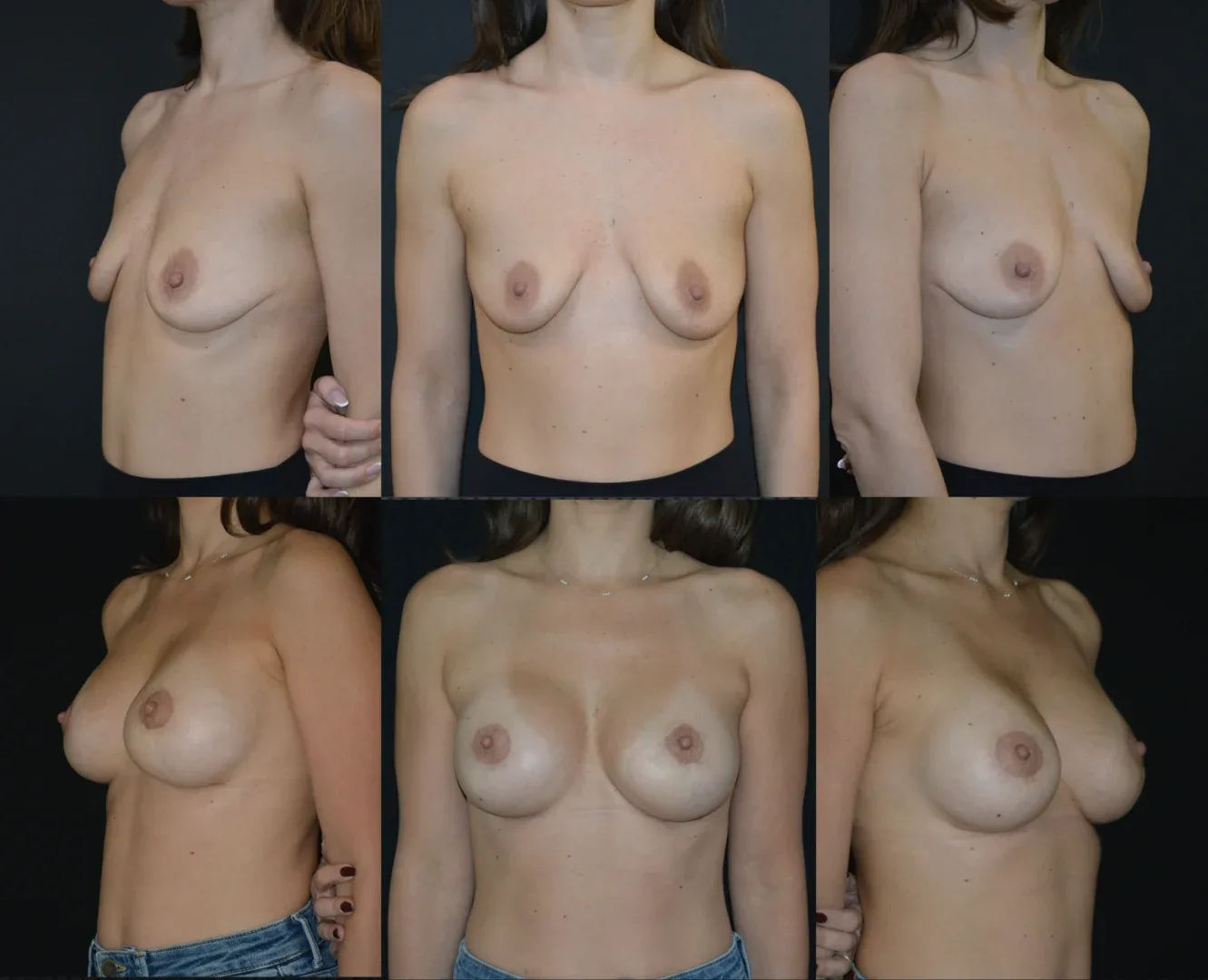
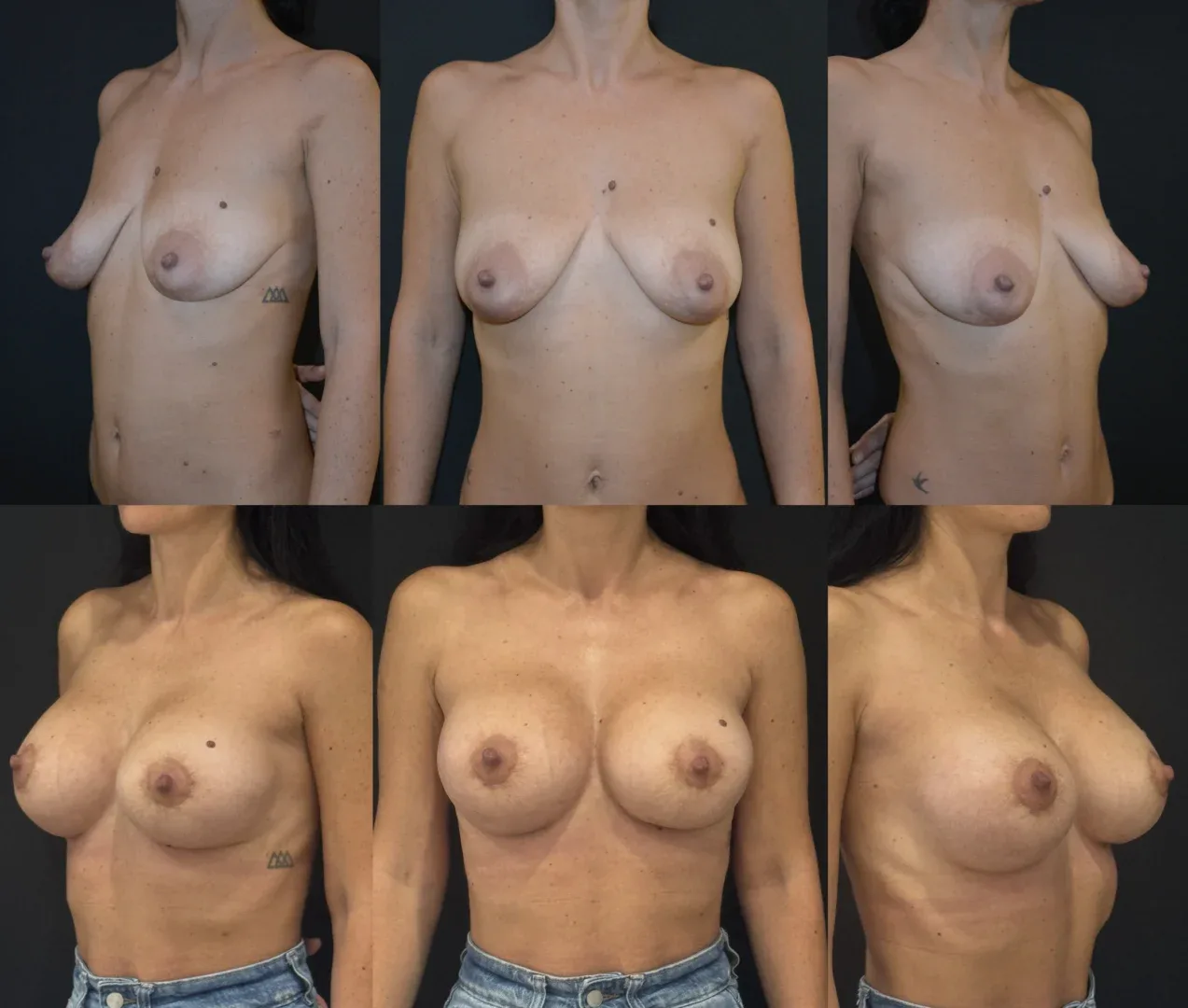
Breast augmentation results are immediately visible. Final results appear gradually over the following weeks as swelling subsides and the breast shape and volume stabilize. Scars fade over about a year.
Internal Mastopexy (Internal Breast Lift)
Redefining Femininity – Modern Breast Augmentation Techniques by Dr. Horia Șiclovan
What is Internal Mastopexy?
Internal mastopexy, or internal breast lift, is an innovative surgical technique that allows lifting and reshaping the breasts from within, without the external scars of traditional lifting.
This technique repositions the breasts into a firmer, more youthful shape while maintaining a natural and proportional look.
Breast Augmentation with Internal Mastopexy – a Perfect Combination
In many cases, implants alone are not enough to achieve the desired result.
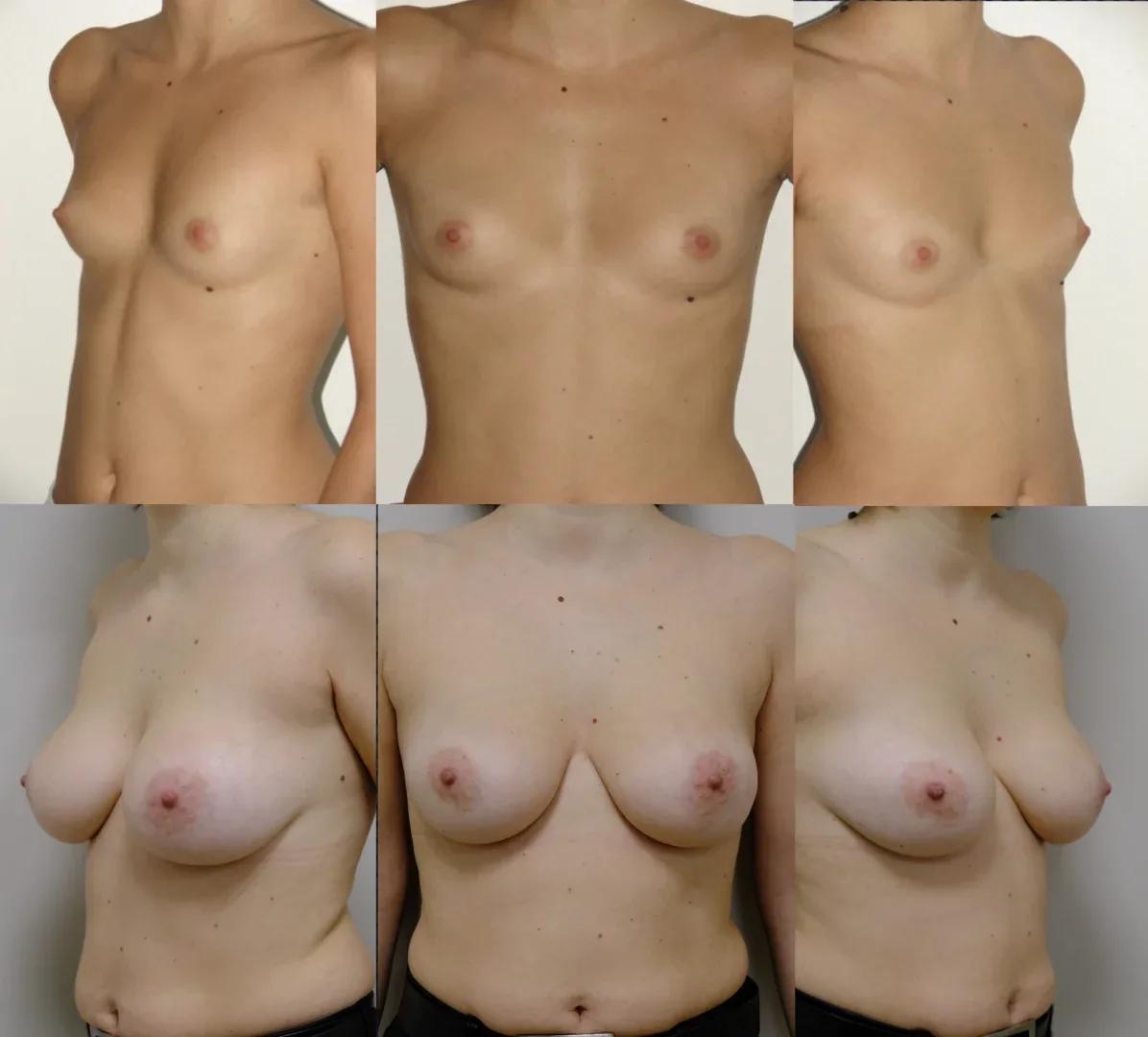
When the skin and tissues have lost elasticity, internal mastopexy combined with augmentation offers the ideal solution: volume, firmness, and correct positioning in a single procedure.
Benefits of Internal Breast Lift
✔️ Natural reshaping with no visible scars
✔️ Stable and long-lasting implant positioning
✔️ Lift effect without additional external incisions
✔️ Faster recovery and minimal discomfort
✔️ Refined aesthetic result adapted to each patient’s anatomy
Original Techniques Developed and Published by Dr. Horia Șiclovan
Based on hundreds of surgeries, I have developed and published two original internal breast lift techniques, recognized for their stability and natural appearance.
MUSCLE SPLITTING BIPLANE TECHNIQUE and INTERNAL LIFT TYPE 1 (see details)
INTERNAL LIFT TYPE 2 TECHNIQUE (see details)
These techniques achieve precise internal repositioning of breast tissue, providing patients with elegant, harmonious, and long-lasting results — without additional scars.
Who is Internal Mastopexy For?
This procedure is suitable for women seeking breast augmentation who present:
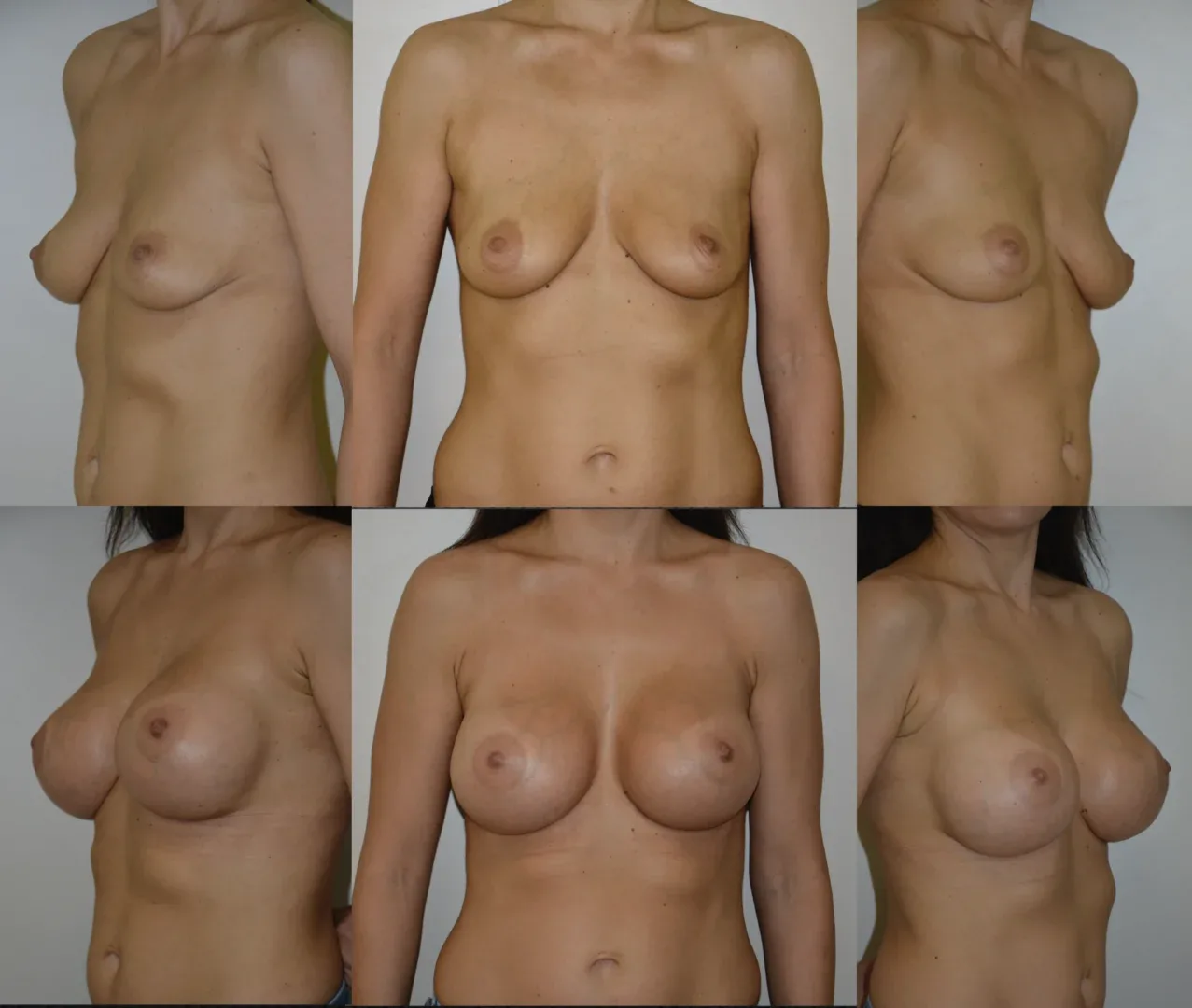
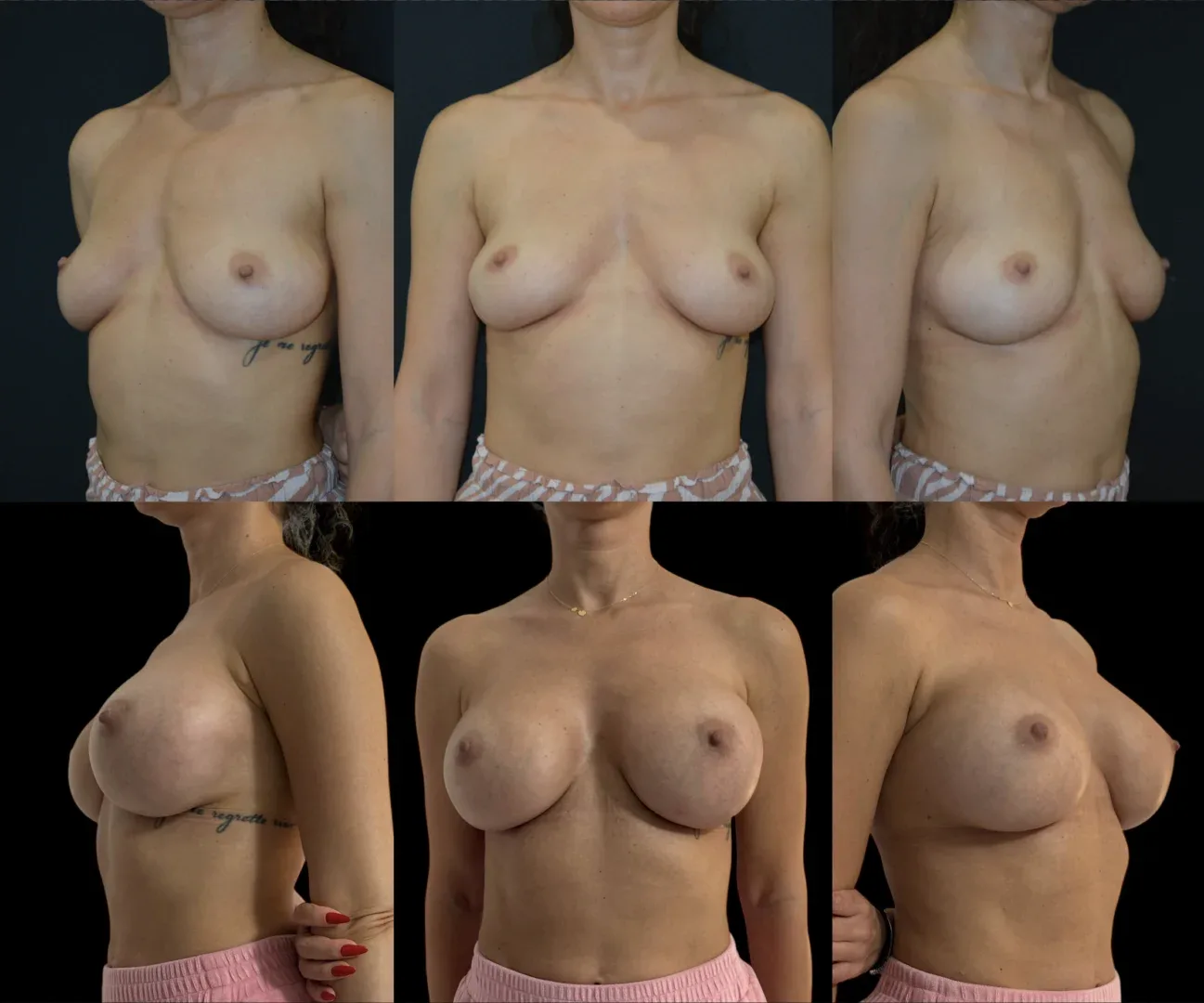
- mild or moderate breast ptosis (sagging)
- asymmetry between the two breasts
- slight skin laxity
- desire to avoid visible scars from classic lifting
Results that Inspire Confidence and Femininity
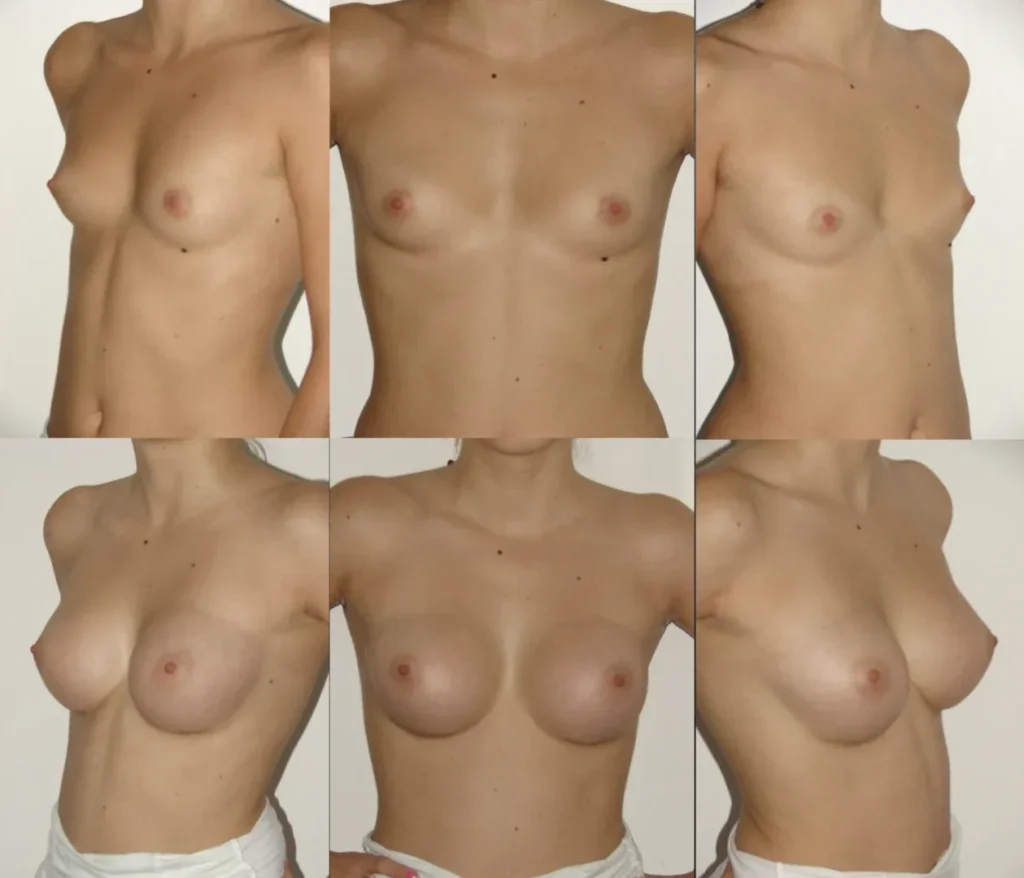
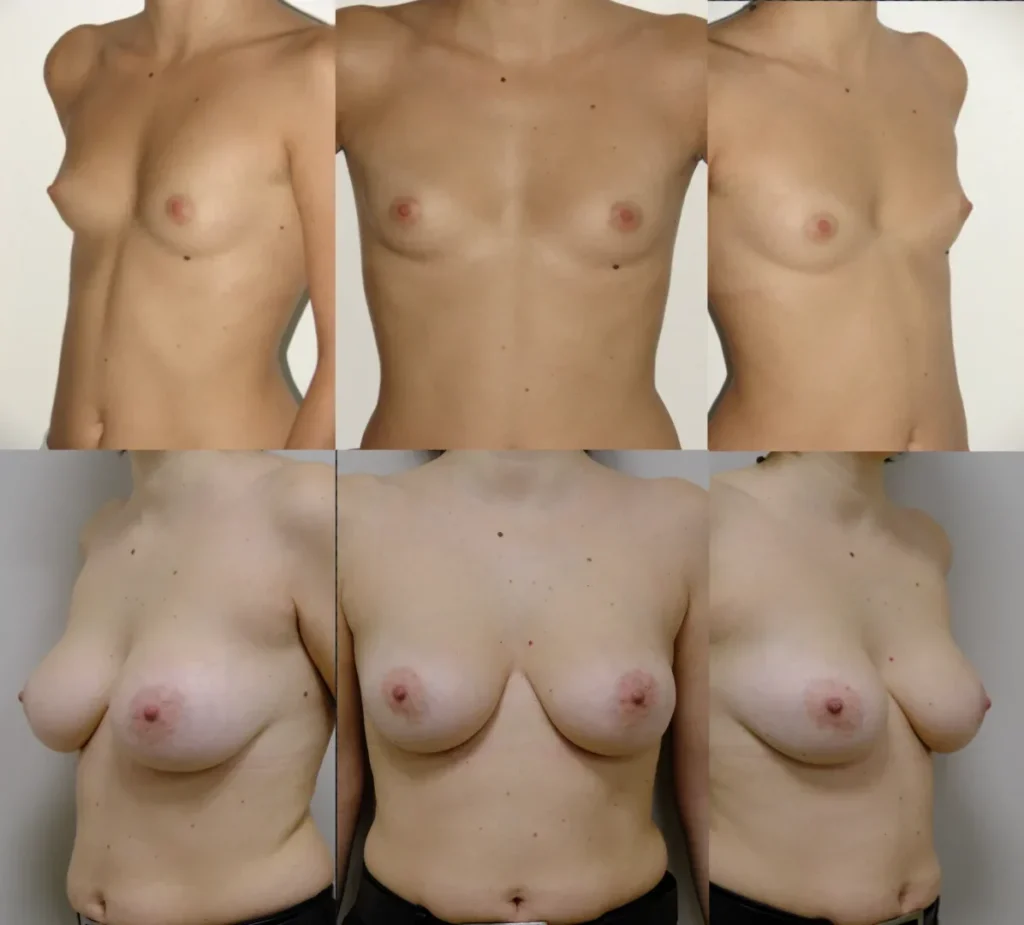
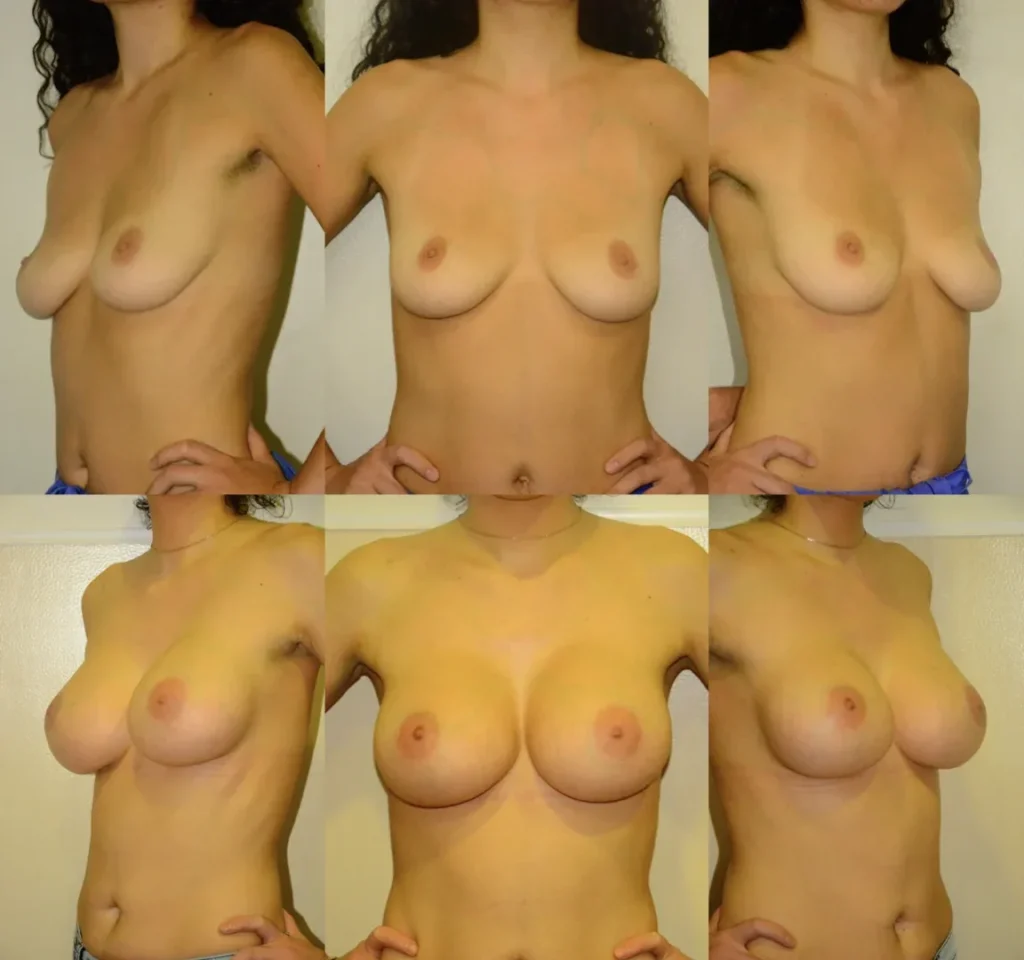
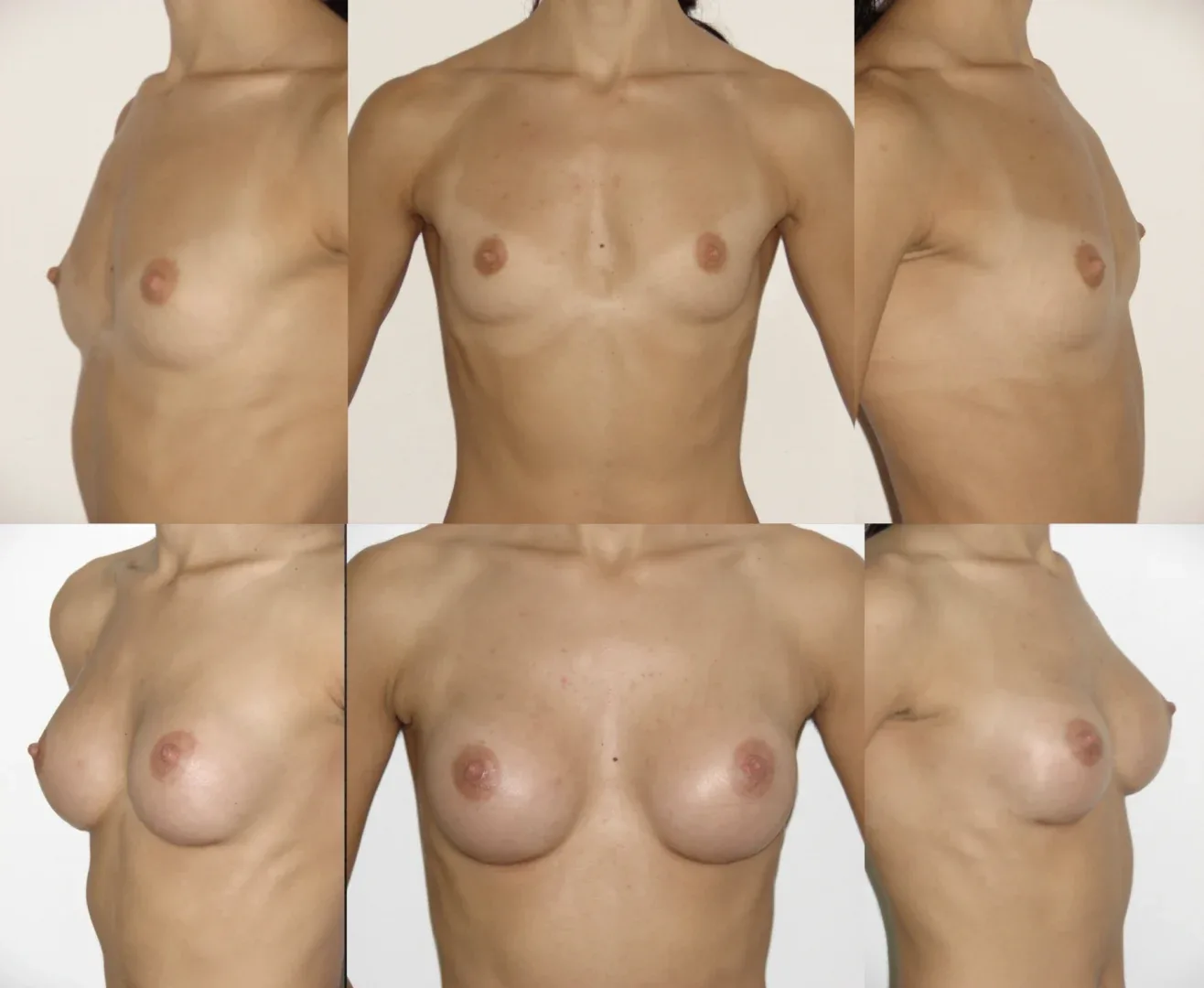
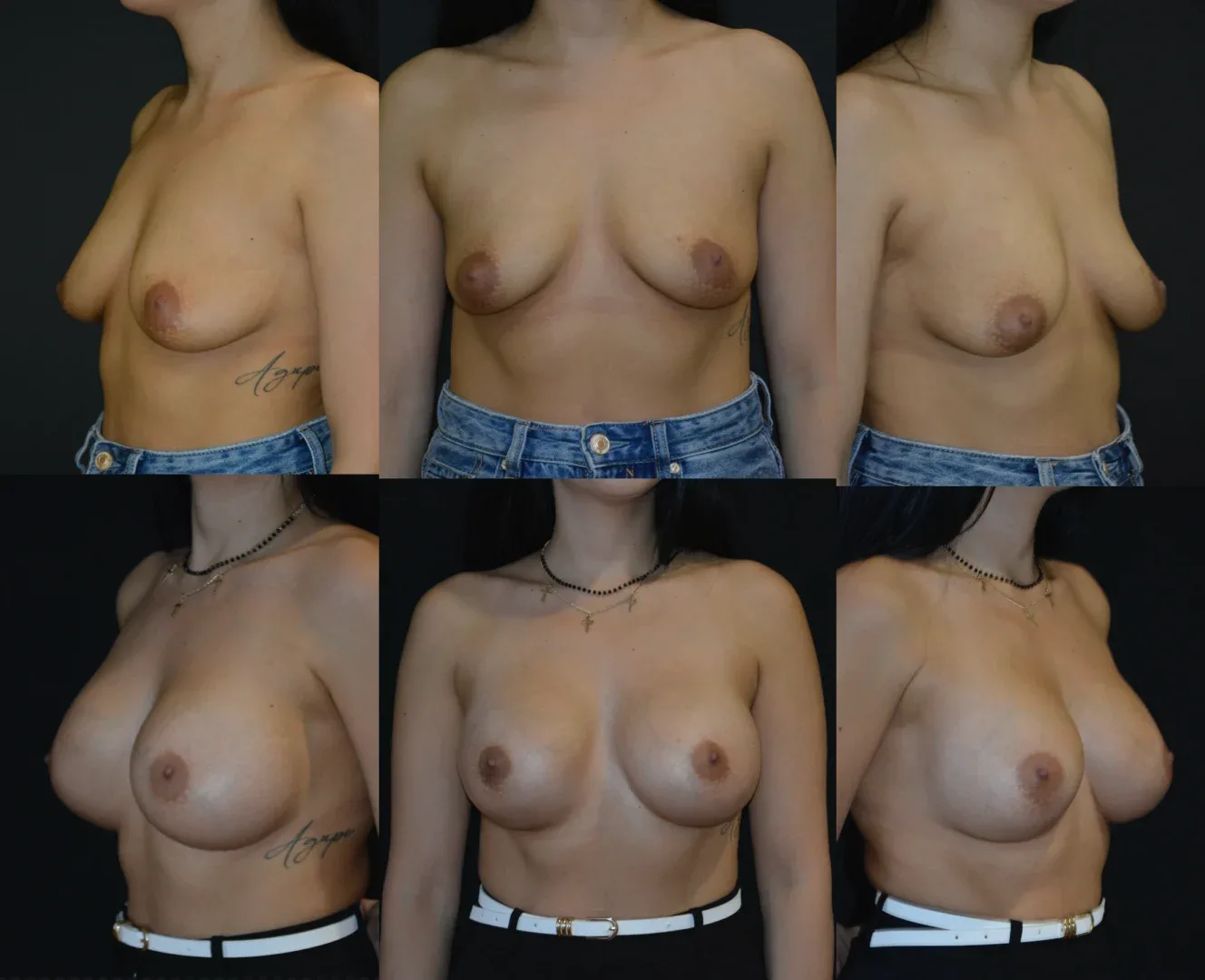
By combining breast augmentation with internal mastopexy, we achieve firmer, younger, and perfectly proportioned breasts, with minimal scarring and long-term stability.
The result is not only aesthetic but also functional — an elegant restoration of body balance and self-confidence.

















































































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}